Article Text

Abstract
Aim To improve medication history accuracy and reduce prescribing errors for unscheduled patients admitted via the emergency department (ED).
Design A prospective observational study of 100 adult unscheduled admissions with 50 patients in both pre and post-intervention groups. One investigator completed the required information including patient demographics, admitting speciality, number and types of any medication errors detected. In the post-intervention group, the investigator (a pharmacist independent prescriber) completed systematic medicine reconciliation in the ED before patient transfer and initiated the original inpatient prescription chart, as appropriate.
Background and Setting The ED in a busy district general hospital with an emergency admission rate of 24 000 patients per annum.
Key Measures for Improvement An increase in medicine reconciliation and initial prescribing within the ED with a reduction in prescribing error rates.
Strategies for Improvement Change needed to be communicated to all staff involved in process: ED medical and nursing staff; appropriate clinical directors; pharmacy staff.
Effects of Change Medicine reconciliation completed within 24 h of admission increased from 50% to 100% and prescription chart initiation in the ED increased from 6% to 80%. The prescribing error rate was reduced from 3.3 errors to 0.04 errors per patient (difference 95% CI 2.5 to 5.1).
Lessons Learnt Streamlining the admission process for unscheduled patients leads to improvement in care, decreases prescribing errors and reduces either potential or actual harm. Moving pharmacists' work to the ED better aligns their input to the patient journey and utilises their knowledge and skills to the patient's benefit.
- ECG
- effectiveness
- emergency department management
- emergency medicine
- major incidents
- medication errors
- medicine reconciliation
- pharmacist independent prescribing
- planning
- resuscitation
Statistics from Altmetric.com
- ECG
- effectiveness
- emergency department management
- emergency medicine
- major incidents
- medication errors
- medicine reconciliation
- pharmacist independent prescribing
- planning
- resuscitation
An accurate medication history is essential to ensure optimum diagnosis and treatment. The difficulty in obtaining this history is well documented.1–7 It may be even more challenging when the process is carried out in relation to an emergency care episode when difficulties are compounded by the involvement of multiple healthcare professionals, increased frequency of hand-offs, and care transferring between geographically discrete areas.
A medication history should include a record of both prescription and non-prescription medicines and an accurate list of allergies.2 7 It has been reported that a quarter of all hospital prescribing errors are the result of incomplete medication histories.4 Evidence suggests that up to 67% of patients' medication histories have one or more errors and up to 46% of medication errors occur when new prescriptions are written at patient admission or discharge.5
It was intended to review the rate of medication errors associated with emergency admission within a busy Scottish district general hospital and subsequently to assess the impact on that error rate with the introduction of medicine reconciliation by a pharmacist independent prescriber within the emergency department (ED), and therefore at an earlier stage in the patient journey.
Background
Crosshouse Hospital is a 552-bed district general hospital with an ED census of 68 000 attendances and approximately 24 000 emergency admissions per year.
The hospital admission process dictates that all emergency admissions are admitted via the ED including general practitioner (GP) pre-assessed patients. One-third of all emergency admissions are GP pre-assessed and two-thirds have not been seen by a GP. All patients are assessed at presentation and undergo modified early warning scoring. If there are no problems with this assessment then the pre-assessed patients progress to the subspeciality bed for further care. Clinical concern will trigger further review within the ED. All patients who have not been pre-assessed are worked up, clerked in, and referred to the relevant subspecialities before admission.
Within the process described, it is possible for the doctor in emergency medicine to record the medication history in the departmental notes, a copy of which would be transferred with the patient to the subspeciality areas. There is access to the emergency care summary (ECS) within the ED.8 A formal prescription chart may be initiated within the ED by emergency medicine staff, although this occurred infrequently and the approach was not standardised.
Occasionally, subspeciality doctors would review patients in the ED and perform traditional clerking and prescription chart initiation within the department.
Junior speciality medical staff on the subspeciality receiving wards would initiate new documentation as part of the traditional medical clerking process. Here, the patients' medication histories would be recorded for the admitting speciality and the prescription chart usually initiated. Previous concerns, including adverse incident reports, had been raised about the completeness and accuracy of the medication history at this stage of the patient journey. This had not been quantified.
Pharmacist review would be carried out in the ward areas, including patient consultations to obtain an accurate medication history. Patients are reviewed at different stages of their journey when a mixture of new patients and established inpatients are present. Errors may be detected at this time. However, this review was not carried out on every admission due to pharmacy staff availability.
Consultant assessment would generally occur later in the patient journey and often involved further changes to medicines. The temporal relationship between the pharmacist review and the consultant ward round, with the majority of patients admitted in the out-of-hours period and consultant post-receiving rounds taking place first thing in the morning, often resulted in senior medical review without the benefit of previous pharmacist review of patient medications. Errors of medicines management may not have been identified and it is possible to potentiate any inherent mistakes.
A systematic review of all the patients' medicines was not standardised within this senior medical ward round. The traditional multidisciplinary admission process lacked a formal medicine reconciliation document, and so any planned changes made to the patients' existing medicines were not recorded in a standardised manner. This had the potential to contribute to confusion and possible errors due to poor communication of intended amendments.
Strategy for change
Medicine reconciliation has been defined by the Institute of Healthcare Improvement as ‘being the process of identifying the most accurate list of a patient's current medicines—including the name, dosage, frequency and route—and comparing them to the current list in use, recognising any discrepancies, and documenting any changes, thus resulting in a complete list of medicines accurately communicated.'9
Systems such as the ECS provide information about what has been prescribed by patients' GPs.8 This should be supplemented by a detailed clinical interview to determine how patients are actually using their medicines and any additional medicines prescribed or purchased.6
Guidance suggests medicine reconciliation should occur within 24 hours of hospital admission, with pharmacist involvement occurring as soon as possible after admission.10 11 A recent study demonstrated that pharmacist-acquired medication histories in the ED had significantly fewer errors.12
It had been identified that the existing process had the potential for resultant prescribing errors and inherent delays in rectifying errors, and that there was a lack of a formal documentation of any planned changes to medicines.
A formal medicine reconciliation form was developed, tested, altered, re-tested and then implemented as part of the required work for the Scottish patient safety programme within the health board area.13 The completed medicine reconciliation form was then used as basis for preparing the initial inpatient prescription sheet. The final form is shown in appendix A.
Measurement of the problem
The study was designed to: ascertain the current level of reconciliation of medicines and prescribing error rates for unscheduled care patients admitted via the ED;and assess the impact on the level of reconciliation and prescribing error rates by the intervention within the ED of the addition of a pharmacist independent prescriber using the recently designed medicine reconciliation form.
This was a prospective observational study of 100 consecutive adult unscheduled care admissions. Patient episodes were examined with 50 patients in both the pre and post-intervention groups. A data collection form was developed with one investigator completing the required information including patient demographics, admitting speciality, number and types of any medication errors detected. Patient medication review was carried out within 24 hours of admission in each case.
Intervention
The investigator (a pharmacist independent prescriber) completed systematic medicine reconciliation in the ED before patient transfer and initiated the original inpatient prescription chart, when appropriate.
A formal medicine reconciliation sheet was compiled to be transferred with the patient from the ED to the receiving ward accompanied by a completed prescription chart.
This change needed to be communicated to all staff involved in process by both investigators:
Medical and nursing staff within the ED informed of pharmacist's role within the study through educational meetings and one-to-one communications.
Information was communicated on the project and proposed change to the clinical directors. This information was cascaded to all medical staff and followed up with direct discussion on specific aspects of medicine reconciliation and prescription chart use.
Pharmacy staff were engaged and informed of the project again through meetings and one-to-one communications.
Measurement of change
Results were collated from data collection sheets with a pre and post-intervention comparison. Unpaired t tests were used to determine whether statistically significant differences existed between the pre and post-intervention groups.
Results
Both the pre and post-intervention groups were similar for patient demographics and the mean number of medicines and are shown in table 1.
Patient demographic details
Admitting specialities were identical for both groups, with the majority of patients transferred to medicine and shown in figure 1.

Admitting specialities.
Appropriate reconciliation of medicines was assumed to be completed if the clinical pharmacist review occurred within 24 h of hospital admission. This occurred in 50% of pre-intervention patients. Post-intervention, all patients had their medicines formally reconciled and documented by one of the investigators in the ED.
The location of prescription chart initiation changed with the intervention from the wards to the ED and is demonstrated in figure 2. For the patients in the post-intervention group who did not have a prescription chart initiated in the ED it was not deemed appropriate for this to have been carried out. Of this group, five patients were following the stroke protocol and were required to be maintained as nil by mouth until they had undergone a formal swallowing assessment. The remaining five patients had oral/subcutaneous medicines changed to the intravenous route in the ED, which necessitated ongoing medical review regarding the continuation or change of route dependent on patient response. In these circumstances a completed medicine reconciliation form was transferred with each patient to facilitate future prescribing.
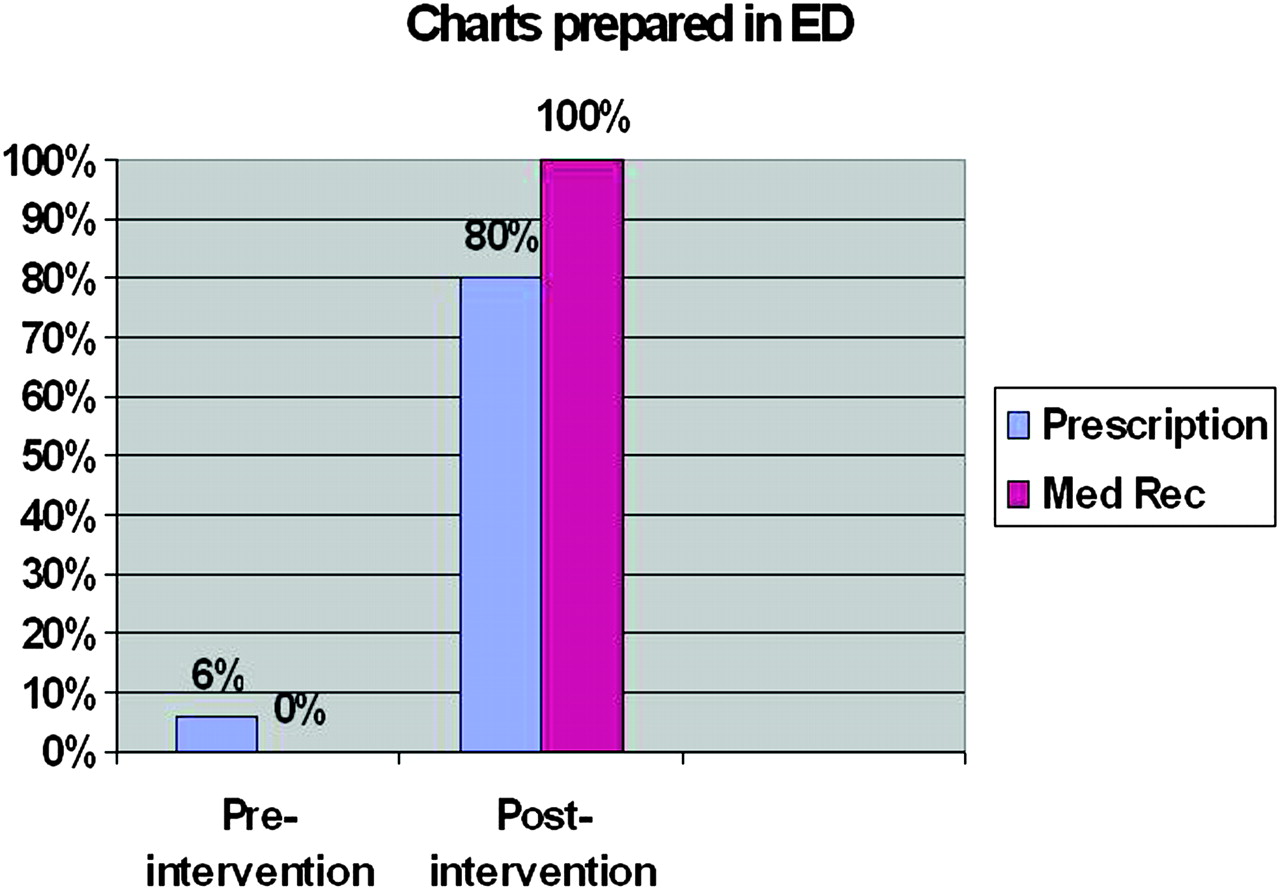
Charts prepared in the emergency department (ED). Med rec, medicine reconciliation form.
Table 2 shows the prescribing errors that were detected and recorded by investigator review 24 h after patient admission. The total number of errors showed a significant difference (difference 95% CI 2.5 to 5.1) with a reduction in errors in the post-intervention group. Failure to use the pharmacist-initiated prescription chart occurred in seven patients in the post-intervention group and contributed to the majority of errors (92%) in the post-intervention patients. This resulted in a similar error rate to the pre-intervention group.
Prescribing errors
In the pre-intervention group, 159 total errors were detected with omissions accounting for the greatest number, demonstrated in figure 3.

{kind=link}
{kind=link}
{kind=link}
Error types.
In the post-intervention group, two errors were detected on review of charts initiated by the investigator. This consisted of one incomplete/incorrect dose and one additional allergy detected on case note review not available in the ED. Twenty-four errors were detected on review of the doctor-created charts on the wards. Again omissions accounted for the greatest number of errors. The different error types and rates of error found in this study are comparable with previous published studies.6–8
Lessons learnt and next steps
Effective planning of change is required and this must be managed. Assessment of existing processes is necessary to define any potential underlying problems that could benefit from a defined process change, linked to the available evidence base relating to medicines reconciliation and prescribing errors. It was clear that there was significant variation in the approach to prescription chart writing and medicines management in general. The planned communication strategy for change implementation appeared to be a successful component in reducing this variation in practice although some persisted. The intervention of independent pharmacy prescribing utilising a formal reconciliation form within the ED clearly reduced the error rate in medicines prescribing.
Clinical impression indicated that the pharmacist involvement had a positive educational effect on prescription writing both in the ED and on the wards, although assessment of this impact extends beyond the scope of this study.
It is important to consider the context of the ED within the hospital as a whole and as a seminal component of the emergency care journey. Streamlining the patient admission process for unscheduled care patients leads to an improvement in patient care and results in a decrease in prescribing errors and a reduction in either potential or actual patient harm.
The redefined process is also a significant advance in providing patient and family-centred care, which is now an organisational priority. Obtaining and documenting the patients' medication history in the ED may have several advantages and directly relate to this strategy. It is possible to consult with the patients' relatives or carers who are frequently present with the patient on hospital arrival. By the time the patients are admitted these relatives or carers may have left the hospital. Often the patients' medicines that have been brought in for admission are returned home before the patient's arrival on a ward. Patients' own medicines are an ideal source for an accurate medication history and may also provide additional information regarding the patient's compliance or ability to use their medicines properly. The location permits prompt prescribing of the patient's medicines at the start of the patient journey, resulting in fewer missed doses associated with the inherent delays that can be present in the emergency care journey. Finally, the ability to access the patients' ECS on receipt of valid patient consent also contributes to the ability to create a detailed and accurate medication history. At present not all junior medical staff have access to the ECS, but all staff working in the ED are permitted access after undergoing suitable training.
As a result of the study it is proposed to introduce pharmacist independent prescribers to the ED to carry out formal medicine reconciliation. Moving the pharmacist work to the ED appears to be an efficient use of resources in that their input is now better aligned with the patient journey. The divergence of the patient journey beyond the ED has made it difficult to deliver this intervention in a consistent manner at a standard time in that journey. In addition, it is important to maximise finite resources to achieve the greatest potential patient benefit. Targeting the knowledge and skills of the clinical pharmacists to align with the patient journey is likely to add the greatest value with early intervention outweighing the later intervention.
For independent prescribing, the pharmacist would be a minimum of band 7 within Agenda For Change. The applicable cost range is £29 789 to £39 273, which contrasts to the cost of a foundation doctor year 2 on a 50% supplement of £41 285. Whether this strategy is adopted as part of a resource re-alignment or as part of a new service development would be a matter for local service design. This change would be set in the context of service improvement including patient safety and the wider quality agenda.
Message for others
The ED is an ideal location for pharmacist involvement in medicine reconciliation for unscheduled care patients. The intervention resulted in quality improvement in medicines information and fewer errors in the initial inpatient prescription chart. These results should be considered in the future emergency care service re-design.
Potential limitations of the study
The study involved a relatively small patient sample, although this is likely to be sufficient for a service improvement study. A single investigator performed the inpatient medication reviews and was therefore assessing their own intervention in the post-intervention group. The standardised data collection form was used to try and mitigate any associated bias. The Hawthorn effect should be taken into consideration when reviewing the results of this study.
Acknowledgments
The authors thank the emergency department, pharmacy department and all ward staff involved for their assistance in this study.
Appendix

Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.