Article Text

Abstract
Objective To characterise the use of interpreter services and other strategies used to communicate with limited English proficient (LEP) patients throughout their emergency department visit.
Methods We performed a process tracing study observing LEP patients throughout their stay in the emergency department. A single observer completed 47 hours of observation of 103 communication episodes between staff and nine patients with LEP documenting the strategy used to communicate (eg, professional interpreter, family member, own language skills) and duration of conversations for each communicative encounter with hospital staff members. Data collection occurred in a single emergency department in the eastern USA between July 2017 and February 2018.
Results The most common strategy (per communicative encounter) was for the emergency department staff to communicate with the patient in English (observed in 29.1% of encounters). Total time spent in communicating was highest using telephone-based interpreters (32.9% of total time spent communicating) and in-person interpreters (29.2% of total time spent communicating). Communicative mechanism also varied by care task/phase of care with the most use of interpreter services or Spanish proficient staff (as primary communicator) occurring during triage (100%) and the initial provider assessment (100%) and the lowest interpreter service use during ongoing evaluation and treatment tasks (24.3%).
Conclusions Emergency department staff use various mechanisms to communicate with LEP patients throughout their length of stay. Utilisation of interpreter services was poorest during evaluation and treatment tasks, indicating that this area should be a focus for improving communication with LEP patients.
- global health
- communications
- patient support
- safety
Statistics from Altmetric.com
Key messages
What is already known on this subject
Interpreter services are underused in emergency medicine, and despite decades of research, our patients with limited English proficiency continue to face quality and safety disparities. Previous studies singularly report interpreter service use as ‘received’ or ‘not received’ and have not studied interpreter service use across the continuum of care in the emergency department.
What this study adds
In this observational study, we found that the use of interpreter services and other strategies (eg, family members) varied greatly across phase of care, with both recommended and non-recommended forms of communication used. The best adherence to professional interpreters occurred during triage and the initial provider assessment, while the poorest utilization was observed during subsequent evaluation and treatment tasks. Ongoing evaluation and treatment tasks include medication administration, obtaining images, sample or vitals collection and follow-up examinations. Underutilization of professional interpreter during these tasks presents challenges to emergency medicine clinicians and can be dangerous to the patient.
Introduction
Background/Rationale
Patient-provider communication is critical to safe and effective care delivery in emergency medicine (EM).1 Successful communication becomes challenging when there is a language barrier between patients and care providers. Language barriers typically occur when a patient cannot effectively communicate in the official language(s) of a given country.
Patients with language barriers experience adverse events more frequently, encounter more severe harm related to adverse events, face poorer quality outcomes (eg, unplanned return to the emergency department) and report significantly lower levels of satisfaction with care.2–4 Unsurprisingly, these inequities have been linked to failures in communication.2 For example, patients with language barriers are twice as likely to be the victim of medical error and have an increased rate of unplanned return to the ED within 72 hours, a widely recognised EM quality metric.2 Research on improving interpreter use and care for patients with language barriers has been conducted for over 30 years, yet appears to be having limited widespread impact; recent studies have demonstrated that quality and safety disparities for patients with language barriers persist.3 5 6
Providing healthcare to patients with language barriers has become increasingly prevalent as global travel and relocation increases. Studies describing the difficulties and deficiencies in providing safe, high quality care to patients with language barriers have been published from countries, including the USA,2 3 Canada,5 Australia,7 Switzerland,8 The Netherlands,9 Belgium,10 and Spain.10 Researchers have also found that persons with language barriers have an increased use of EM services, making this issue particularly prevalent in EM.11
Many countries recommend or mandate the use of professionally trained interpreters.7 12 13 Use of certified professional interpreters has been found to improve communication, increase patient satisfaction and improve quality of care.4 14 15 Increased availability in telephone and video-based platforms have improved interpreter access, but barriers to the consistent utilisation still exist.5 7 14 Studies from Canada,5 New Zealand,7 Australia7 and the USA report the underutilisation of professional interpreters.15 Studies in an EM setting have estimated rates professional interpreter services use between 12% and 32%.15 16 It is, however, unclear what these percentages mean in an EM context where several staff members communicate with patients on multiple occasions.
Previous studies regarding interpreter service use in the ED have relied on postencounter surveys or electronic documentation reports. These methods do not capture the multitude of encounters that occur between patients and ED staff members. In order to better understand interpreter service use across the continuum of care, this study involved observation of ED patients throughout their length of stay to quantify how interpreters were used to communicate with patients with language barriers. The results can allow us to propose methods for systematically improving communication with patients with language barriers.
Methods
Study design and setting
This research used a cross-sectional, observational study of patients with language barriers (Spanish-speaking) throughout their course of stay in the ED. For the purposes of this study, which occurred in the USA, patients with language barriers are specifically referred to as patients with limited English proficiency (LEP). Spanish-speaking patients were chosen because they represent the largest proportion of LEP patients in the given study setting and the USA as a whole; 65% of the US LEP population speaks Spanish.17 Observations were conducted in a single urban, adult, tertiary care ED. The ED has an annual patient census of approximately 90 000 patients. The ED is staffed by employed nurses, patient care technicians, physician assistants, EM attending physicians, EM resident physicians and internal medicine resident physicians. The study site was located in the Eastern USA, and observations occurred between July 2017 and February 2018.
The hospital is staffed by in-person, Spanish-speaking interpreters from 07:00 hours through 20:00 hours Monday-Friday. Four interpreters work staggered, 8 hour shifts during this time period and are a shared resource throughout the hospital that the ED can access depending on availability. When in-person interpreters are not available, ED staff can use a telephone-based interpreter service that the hospital subscribes to.
Participants
Participants were recruited on entry to the ED. The observer identified Spanish-speaking patients during their registration by listening to their conversations with the intake clerk. The observer then approached the patient, confirmed they spoke Spanish and that they needed an interpreter and then explained the study and consent materials. Consent materials had been professionally translated into Spanish. Potential participants voluntarily elected to participate by providing verbal consent.
This study was approved by the healthcare system’s institutional review board.
Measurement
A single observer (author NCB) conducted all observations. The observer had over 100 hours of experience conducting observations in the ED and has professional working proficiency in the Spanish language. Observations were stratified across three time periods: weekday mornings (before 12:00 hours), weekday afternoons (12:00 hours to 20:00 hours) and weekday evening (after 20:00 hours)/weekends. The stratification was designed to sample a variety of situations and contain scenarios where in-person interpreters were not available (weekday evenings/weekends). Participants were also balanced across care area (fast track vs main ED) to obtain a variety of patient acuity levels.
Observational data collection began after participants consented to the study. The observations concluded when one of three criteria were met:
Participant was admitted to the hospital.
Participant was discharged.
Observation time reached over 8 hours.
The observer shadowed participants throughout their stay in the ED, collecting data via pen and paper. Notes were structured similar to a written transcript (ie, beginning time stamp, speaker, information communicated, end time stamp) using loose-leaf paper to facilitate capture annotations and passages of information of varied lengths. Data collection occurred during instances when the hospital staff members were communicating with the participant. Any instance of exchange in information between hospital staff and patient was considered a communicative encounter. Situations where participants were communicating with other people accompanying them (eg, family members) were excluded.
Data elements collected included beginning and end time stamp of the communication exchange, hospital staff member role, strategy used for communicating with the patient (eg, in-person interpreter, patient family), phase of care and the content of the information exchanged (not included in this article). For the purposes of this study, communication strategies encompass any mechanism used to communicate an LEP patient, including one’s own language skills (eg, English, Spanish, verbal communication).
When the hospital staff member did not use a third party (eg, professional interpreter) to facilitate communication, the observer noted whether the hospital staff member communicated with the patient by
Speaking English.
Speaking Spanish (concordant)—meaning the hospital staff member was proficient in Spanish.
Speaking Spanish (partially concordant)—meaning the hospital staff member spoke some words in Spanish but was not proficient.
Quantitative variables
Outcome measures describe the strategies used for communicating with LEP patients throughout their stay in the ED. Primary outcome measures include the percentage of communicative encounters where a given communication strategy was used and the percentage of time (in minutes) a given communication strategy was used. As applicable, these measures were broken out across phase of care. Strategies were categorised according to whether they are recommended by the National Standards for Culturally and Linguistically Appropriate Services (CLAS) in Healthcare.12
Analysis
Following observations, data were entered into structured fields in an excel spreadsheet. Descriptive statistics related to the aforementioned measures were calculated, and visualisations were created using R software (R Foundation for Statistical Computing, Vienna, Austria).
Results
Characteristics of study participants
Nine LEP (Spanish-speaking) patients were observed, resulting in 47 hours of data collection. Table 1 provides details regarding the observation start time, end time, duration, care area, disposition decision and whether or not someone accompanied the patient during their stay.
Summary of observations and participant characteristics
Main results
During the 47 hours of observation, 8.9 hours of communicative encounters (time where hospital staff and LEP patient participants were exchanging information) were observed for a total of 103 encounters. Eight different strategies were used for communication. Table 2 defines each strategy and identifies if these mechanisms are recommended by the National Standards for CLAS in Healthcare.12 Each patient received communication using at least two and as many as five of the strategies listed in table 2. All nine patients observed received communication using at least one type of recommended strategy (ie, a professional interpreter or clinician proficient in the patient’s language) and one type of communication strategy not recommended (table 2).
Description of communication strategies used for exchanging information with LEP patients
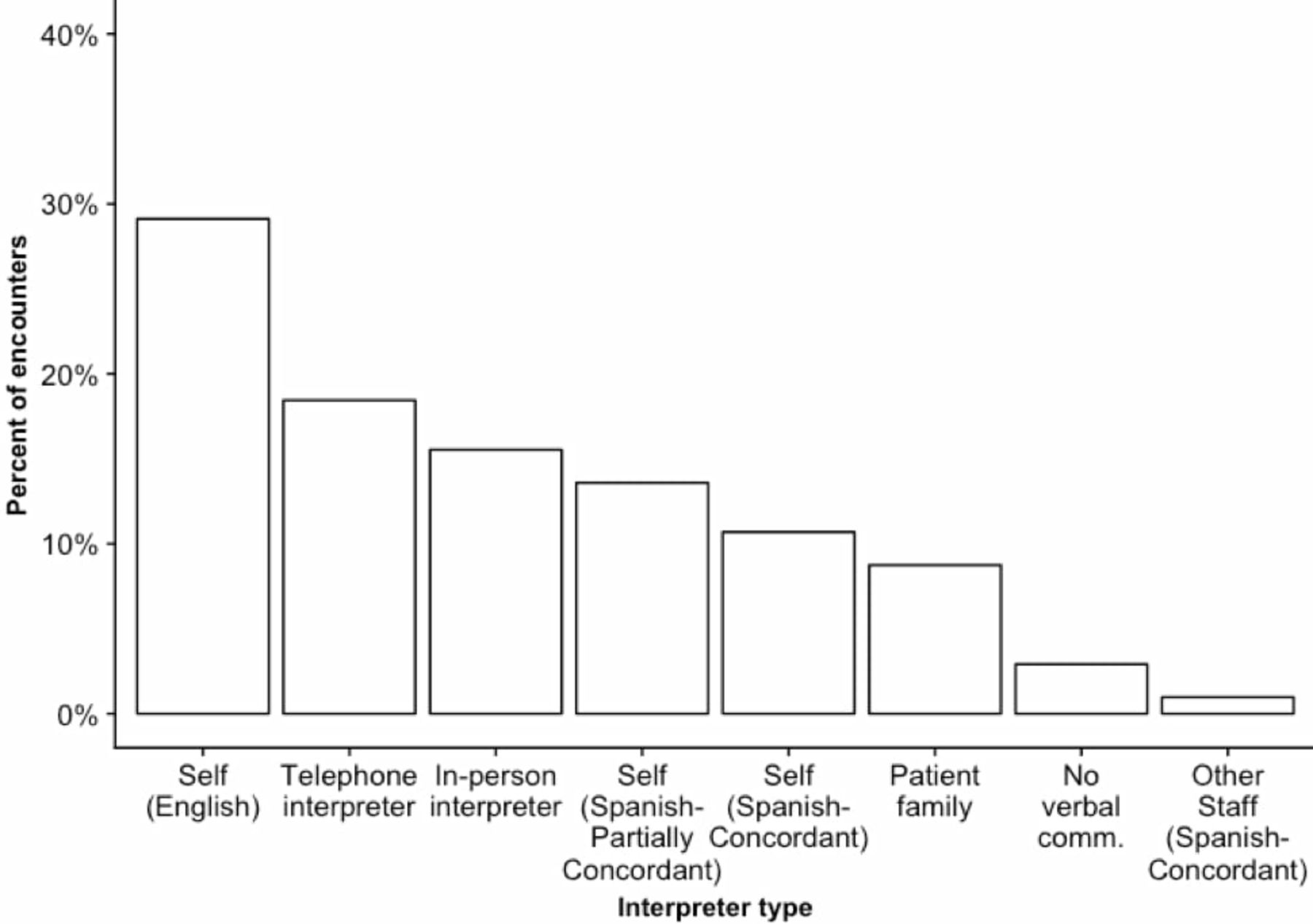
Figure 1 depicts the frequency with which each communication strategy was used across the 103 communicative encounters observed. As demonstrated, the most common strategy was to communicate with the patient themselves in English (not recommended), followed by use of a telephone interpreter, then use of in-person interpreters.
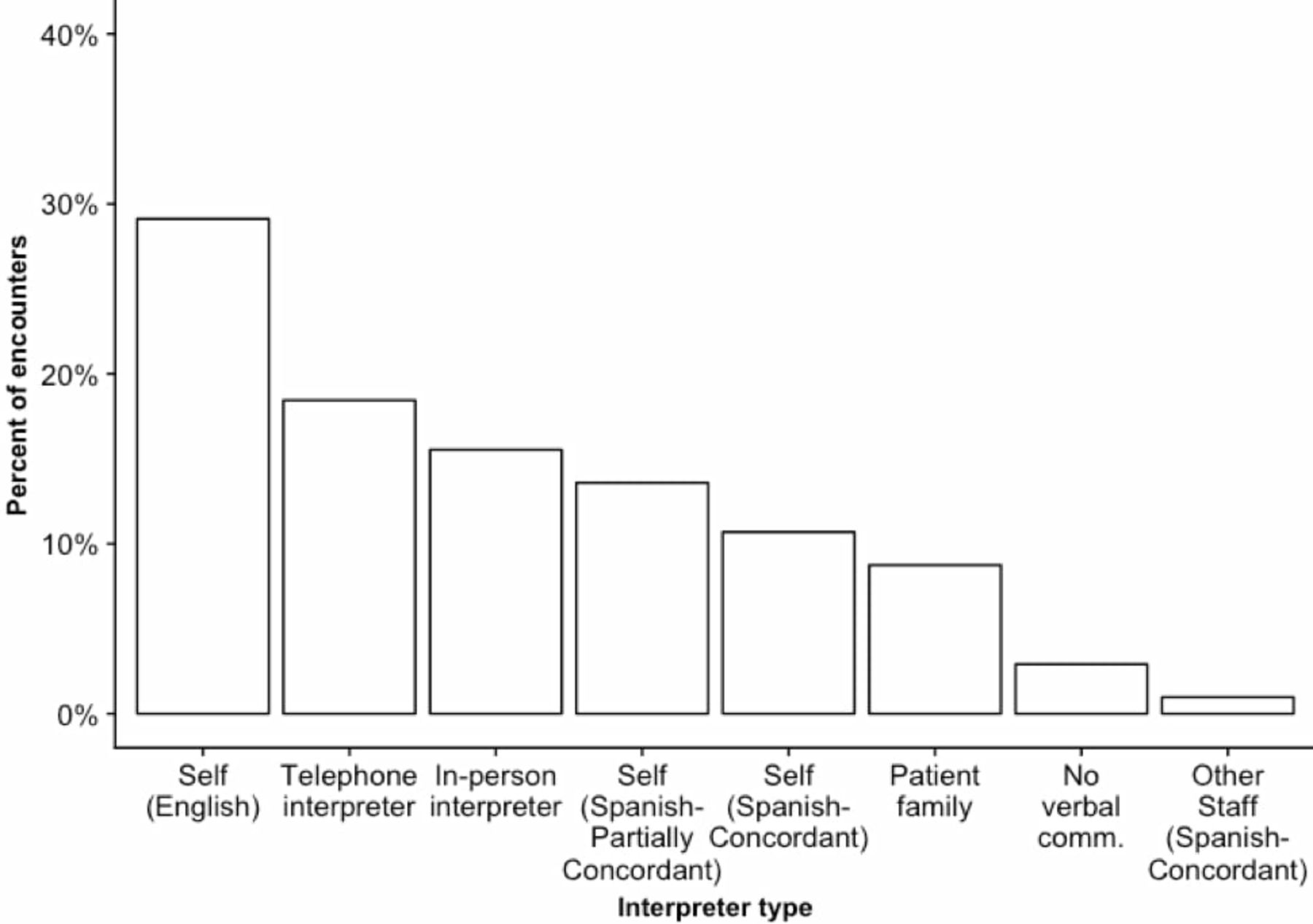
Frequency of each communication strategy used among 103 encounters.
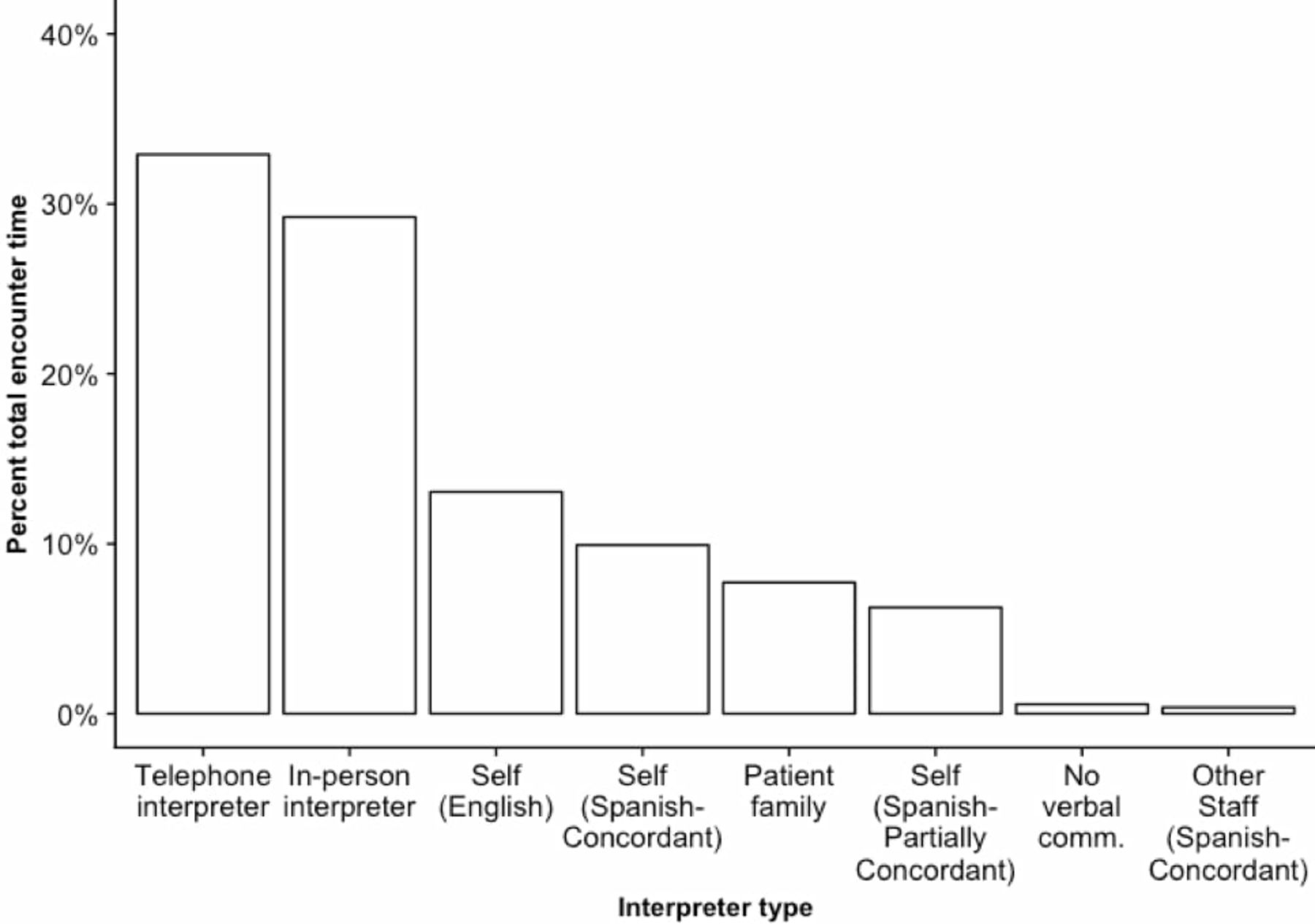
The next analysis considered the amount of time (rather than frequency) with which each communication strategy was used. Figure 2 shows the percentage of total time communicating that each communication strategy was used. A professional interpreter (in-person or telephone-based) or a Spanish-concordant staff member were used for over 70% of the total time spent exchanging information with patients.

Communication strategy use based on duration of encounter (total time spent using each strategy).
The third analysis grouped encounters based on the clinical task executed or phase of care. The phases of care were triage, initial nurse assessment, initial provider assessment, ongoing evaluation and treatment, disposition and registration (which can occur any time after triage but typically occurs in the latter phases of the patients’ stay). The ‘ongoing evaluation and treatment’ phase encompassed any encounters that occurred between the initial assessments and disposition, including consultation; medication or treatment administration; vitals or sample collection; patient examination, preparation or procedure and imaging.
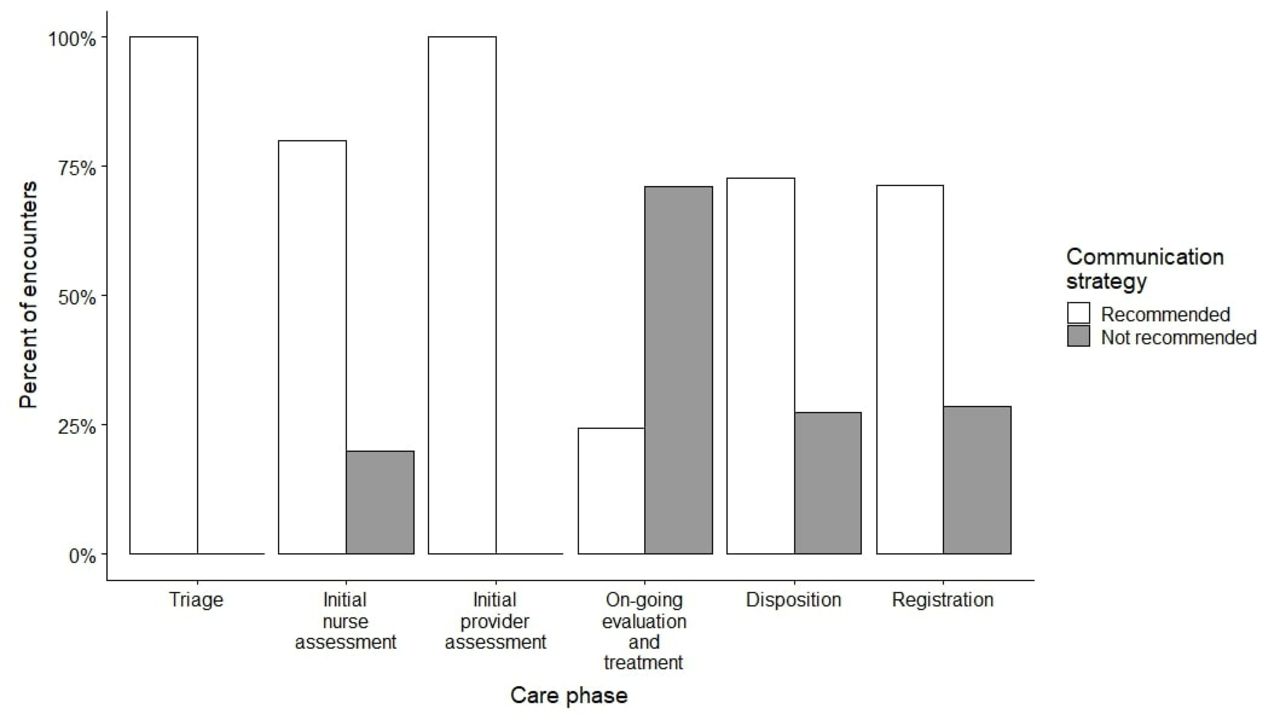
Table 3 provides a detailed breakdown of the communication strategies used (by encounter, similar to figure 1) across phases of care and by the acceptability of each communication mechanism based on the National CLAS Standards.12 Figure 3 summarises the results from table 3 by aggregating all of the formats recommended and not recommended by the National CLAS Standards.12 We found that professional interpreters and language concordant staff members were consistently used during triage, initial nurse assessment, initial provider assessment and disposition. However, during the ongoing evaluation and treatment phase (between the initial assessments and disposition decision), communication often did not include the use of professional interpreters or language concordant staff.

Communication strategy (recommended or not recommended form) broken out by phase of care.
Use of interpreters by encounter across phases of care
To provide a more detailed view of communication, visualisations showing communication strategy use throughout the patients’ length of stay were created. Detailed length of stay visualisations for three representative patient cases with varied levels of complexity are provided. The cases include a patient sent to the fast-track area and discharged (figure 4A), a patient sent to the main ED that was admitted for surgery (figure 4B) and a patient sent to the main ED and discharged (figure 4C).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Visualisations of communication strategy use during the entire length of stay for three representative cases.
These visualisations demonstrate that professional interpreters and language concordant staff members were used more frequently and for longer times in the earlier phases of care and towards the end of the patient’s stay (during disposition). On the other hand, conversations (occurring between initial assessments and disposition) were shorter and used communication strategies that have been demonstrated in other studies to be less effective and are not recommended by national standards.12 15
Discussion
Previous studies have demonstrated a disconnect between the benefits of professional interpreters and the underutilisation of their services.14 18 Barriers to using interpreters services have been identified, including poor identification of when an interpreter is needed, perceived time constraints, financial costs related to interpreter use, lack of available interpreters, loss of control over the communication process and lack of confidence in the accuracy of interpreted dialogue.19 20 These reported barriers, however, have not been contextualised in the continuum of care in EM.
This observational study conducted in an ED identified three key emerging themes in how different strategies are used to communicate with LEP patients in the ED:
Various types of strategies were used to communicate with LEP patients.
Multiple strategies were used to communicate with a single patient.
The communication strategy used varied across phase of care.
First, ED staff used various different strategies (eight observed) to communicate with LEP patients. Four strategies involved the use of different personnel (eg, professional interpreters, family members) and four included communicating with the patient themselves in variations of another language (Spanish), English or via non-verbal communication. ED staff employed these strategies with varied frequencies (per encounter) and for different durations of time. Specifically, staff communicated with the patient themselves in English in nearly 30% of encounters observed, but LEP patients received either a professional interpreter (in-person or via telephone) or a Spanish proficient staff member in over 70% of the total time (in minutes) observed. This finding may signify that staff members tended not to invite an interpreter for conversations they presumed would be short. Alternatively, conversations may have been shorter because an interpreter was not involved
Second, individual patients experienced multiple forms of communication assistance. Every patient observed received either a professional interpreter or communicated with a Spanish concordant clinician at some point in their stay. Each patient, however, encountered at least two and as many as five different communication strategies, and all patients received communication via strategy not recommended by national standards. This demonstrates that reporting professional interpreter use for LEP patient encounters as a dichotomous variable (did receive/did not receive) is an oversimplification of what occurs in reality. Future research should reconsider how interpreter service use could be more accurately captured without creating significant, additional documentation for EM clinicians.
Third, this study found that professional interpreters were well-used in the early phases of care (triage, initial nurse assessment and initial provider assessment) as well as during disposition, but not during the intermediate evaluation and treatment phase.
Conversations that occurred in the evaluation and treatment phase, where staff underused professional interpreters, were typically shorter in duration. In previous studies, clinicians have reported time constraints as one significant barrier to interpreter service use.19 Poor use during shorter conversations, as demonstrated here, may indicate that providers view the time cost of obtaining an interpreter too great for the shorter conversations. Alternatively, conversations during this phase may have been shorter because professional interpreters were less frequently used, allowing for less back-and-forth communication between the staff member and patient. The type of tasks that occur during the evaluation and treatment phase (eg, imaging, medication administration) may necessitate that ED staff and patient have their hands free, making it challenging to use telephone-based interpreters.
Limitations
This study had limitations related to the sample, language proficiency assessment and using a single study site. While the sample size of study participants was limited to 9 LEP patients, the observations represented over 47 hours of data collection and more than 100 communicative encounters. Observations were also stratified across time of day and balanced across care area (fast-track vs main ED) to observe a variety of situations and patient acuity levels. The fact that all patients had similar experiences suggests that the findings are reproducible and this can serve a hypothesis generating for further research. However, encounters with acutely ill patients were not observed and require additional consideration.
During the study, language proficiency of the patients and hospital staff members was not formally assessed. However, the observer (NCB) has professional working proficiency in the Spanish language, allowing a subjective assessment of the staff’s Spanish proficiency.
Observations were collected from a single ED. Because of this, the data should be interpreted for patterns in interpreter use and is not generalisable to determine the raw frequency of interpreter use across given situations. It would be beneficial to conduct studies in additional EDs, and the value of this study is to establish initial trends that might inform the development of improvement efforts for interpreter use and LEP patient communication in the ED.
Recommendations
Our findings suggest ways that the use of interpreter services could be improved in emergency departments.
It would be useful to make hands-free technology available to allow interpretation during encounters where the patient and/or care provider must also have their hands free. The use of high quality speaker-phones or blue-tooth headsets or other hands-free options may streamline the process of obtaining telephone-based interpreter services. Using a hands-free device, the clinicians could also provide information to the interpreter service (eg, hospital location, patient medical record number) while beginning to examine the patient or prepping materials.
The use of video-based services has become increasingly prevalent and has been demonstrated, in some cases, to improve patient understanding as compared with telephone-based services.21 Video-based interpreters are typically provided on movable tablets or carts which may improve the ease of use for scenarios movement is necessary. However, both hands-free telephones and video-based solutions still involve obtaining a piece of equipment and connecting to an interpreter, so issues related to the time-cost of obtaining and interpreter may persist.
It may also be fruitful to explore the development of non-human interpreter tools, especially for conversations where obtaining an interpreter may be less feasible, such as the conversations in the evaluation/treatment phase or for high acuity patients that require immediate care. Many have lauded translation machines, such as Google translate, but recent studies indicate this technology is not yet accurate enough for safety critical domains, such as medicine.22 Medical translation applications, such as the canopy, have been developed; however, further studies are needed to determine if these tools are efficient, effective means for LEP patient communication in a live clinical environment.23 Future tools developed for communicating with ED patients should be contextually appropriate for EM, convey information in both the patient and clinician’s language for shared awareness, be easy and efficient to use and have built-in functionality to obtain a professional interpreter that may be triggered by the patient or clinician if the application is not sufficiently sophisticated for the task at hand.
The depictions of individual patient stays in the ED (figure 4A-3C) highlight the amount of waiting time patient has where they are not interacting with a hospital staff member. It may be beneficial to use this time to educate the patient regarding their rights to interpreter services and the types of services available. Other studies conducted in an EM setting have demonstrated that short, educational videos can improve patient understanding of ED processes and patient satisfaction.24–26 Such videos for LEP patients may help patients and persons accompanying them advocate for the use of interpreters and improve the decreased satisfaction that has been reported by LEP patients in other studies.
The results of this study provide an enhanced understanding of how interpreters are used across the continuum of care in EM and raise hypothesis-generating questions around the finding that under-utilisation lies predominantly outside of the initial assessment conversations. To fully characterise interpreter use, future studies should study interpreter use across the continuum of care in EM due to the various touch points of communication that occur. Solutions to improve interpreter use should involve stream-lining these services so they are more readily accessible for intermittent, shorter encounters as well as exploring the development of non-interpreter-based solutions that may be more feasible for use during shorter, less complex encounters.
References
Footnotes
Contributors NCB and AMB conceived the study with input from RJF, LL and DJH. All authors contributed to optimisation of methods. NCB completed data collection. NCB analysed the data with iterative guidance from RJF, LL, DJH and AMB. NCB drafted the manuscript under the advisement of AMB. All authors contributed substantially to its revision. NCB takes responsibility for the manuscript as a whole.
Funding NCB was supported by the National Science Foundation’s graduate research fellowship program (1117218). This work was also supported by the Charles and Mary Latham Foundation.
Competing interests None declared.
Ethics approval This study was approved by the MedStar Health Research Institute’s institutional review board (Hyattsville, Maryland, USA), protocol #2016-099.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice When this article first published, the title contained an error. It previously read ’Observational study to understand interpreter service use in the emergency medicine…' The use of ’the' has been removed.
Patient consent for publication Not required.