Article Text

Abstract
Objectives To compare infarct size and left ventricular ejection fraction in patients with non-ST-elevation myocardial infarction (NSTEMI) with and without acute coronary occlusions, and determine if myocardial strain by speckle-tracking echocardiography can identify acute occlusions in patients presenting with non-ST-elevation acute coronary syndrome (NSTE-ACS).
Methods 111 patients with suspected NSTE-ACS were enrolled shortly after admittance. Echocardiographic measurements were performed a median of 1 h (interquartile range 0.5–4) after admittance, and coronary angiography 36±21 h after onset of symptoms. Territorial longitudinal and circumferential strain was calculated based on the perfusion territories of the three major coronary arteries in a 16-segment model of the left ventricle, and compared with traditional echocardiographic parameters. Long-term follow-up was by echocardiography and contrast-enhanced magnetic resonance imaging (ceMRI).
Results Patients with NSTEMI due to acute coronary occlusion had higher peak troponin T than patients with NSTEMI without acute occlusions (4.9±4.7 vs 0.9±1.1 μg/l, p<0.001), larger infarct size by ceMRI (13±8% vs 3±3%, p<0.001) and poorer left ventricular ejection fraction (48±6% vs 57±6%, p<0.001) at follow-up. Territorial circumferential strain was the best parameter for predicting acute coronary occlusion. A territorial circumferential strain value >−10.0% had 90% sensitivity, 88% specificity and area under the curve=0.93 for identification of acute occlusions.
Conclusions Patients with NSTEMI due to acute coronary occlusions develop larger infarcts and more impaired left ventricular function than patients with NSTEMI without occlusions, regardless of infarct-related territory. Territorial circumferential strain by echocardiography enables very early identification of acute coronary occlusions in patients with NSTE-ACS and may be used for detection of patients requiring urgent revascularisation.
- Coronary angioplasty (PCI)
- risk stratification
- acute coronary syndrome
- coronary artery disease (CAD)
- NSTEMI
Statistics from Altmetric.com
- Coronary angioplasty (PCI)
- risk stratification
- acute coronary syndrome
- coronary artery disease (CAD)
- NSTEMI
Introduction
Acute coronary occlusion is a common finding at coronary angiography in acute coronary syndromes (ACS).1 2 However, revascularisation strategy is guided by ECG, which has limited sensitivity for identification of acute occlusions.3 In non-ST-elevation ACS (NSTE-ACS), urgent coronary angiography is recommended only for patients with high-risk features, a group representing a small proportion of the patients.4
Non-ST-elevation myocardial infarction (NSTEMI) with an occluded infarct-related artery probably shares the same pathophysiology as myocardial infarctions with ST elevations (STEMI)5 and these patients may be at risk of extensive myocardial injury if flow is not rapidly restored. However, early risk stratification in NSTE-ACS is difficult. Myocardial strain by echocardiography enables evaluation of global and regional myocardial deformation and can identify abnormal function due to ischaemia and necrosis.6–13 Echocardiography is easily accessible and can be performed at the bedside in an emergency setting. Consequently, strain determined by echocardiography may be a feasible method for early identification of acute coronary occlusions in patients with NSTE-ACS.
The aims of this study were to compare outcome as measured by final infarct size and left ventricular (LV) function in patients with NSTEMI with and without acute coronary occlusions, and to determine if territorial strain might be used for very early identification of acute coronary occlusions in NSTE-ACS.
Patients and methods
Patients
Patients with suspected NSTE-ACS admitted to a local hospital were consecutively evaluated for study inclusion. Eligible patients had to fulfil three criteria: acute anginal pain lasting for ≥10 min, a history of <3 days and indication for coronary angiography according to guidelines.4 Exclusion criteria were: age <18 years, history of myocardial infarction, previous open chest surgery, bundle branch block, severe valvular dysfunction, atrial fibrillation with heart rate >100 bpm or continuous severe arrhythmia, or any condition which interfered with the patients' ability to comply. The study population comprised 111 patients with suspected NSTE-ACS with planned coronary angiography. All patients received medical treatment according to the guidelines.4 NSTEMI was diagnosed by convention, using a cut-off value of troponin T >0.03 μg/l,14 whereas unstable angina was defined as NSTE-ACS with troponin T ≤0.03 μg/l. Patients without ischaemic ECG, troponin T elevation or significant coronary artery stenoses were classified as non-coronary chest pain. Troponin T was determined at admittance, after 6–8 h, twice daily, before coronary angiography and 2 and 24 h thereafter. Standard ECGs were carefully analysed by experienced cardiologists. TIMI and GRACE risk scores were calculated for all patients.15 16
Retrospectively, all patients with suspected NSTE-ACS were grouped according to whether the culprit lesion was occluded or non-occluded. These groups were compared and the ability of clinical and echocardiographic parameters to identify acute coronary occlusions at admittance evaluated. In addition, patients with NSTEMI were assessed separately to evaluate the consequences of acute coronary occlusions on long-term outcome.
The research protocol was approved by the Southern Norway Regional Committee for Medical Research and Ethics. All patients provided written informed consent.
Echocardiography
Echocardiographic examinations were performed with a Vivid 7 scanner (GE Ultrasound, Horten, Norway). Recordings were digitally stored. Measurements were performed a median of 1 h (interquartile range 0.5–4) after admittance. Patients with NSTEMI were re-examined 98±21 days after admittance. Three consecutive heart cycles from three apical planes (four-chamber, two-chamber and long-axis) and three short-axis planes (mitral, papillary and apex) were obtained by two-dimensional grey-scale echocardiography. Frame rate was 74±9 frames/s. These images were used for both conventional and strain analyses. LV end-diastolic volume and ejection fraction (LVEF) were assessed by the Simpson biplane method.17 Wall motion score was visually assessed in a 16-segment model, as normal=1, hypokinetic=2, akinetic=3, dyskinetic=4.17 The wall motion score index (WMSI) was the average value of analysed segments. All echocardiographic and strain recordings were analysed separately by a single observer blinded to other patient data, using EchoPAC version 7 (GE Ultrasound).
Strain analyses
Myocardial strain was measured using speckle-tracking echocardiography. Territorial strain was calculated based on the perfusion territories of the three major coronary arteries in a 16-segment LV model,18 by averaging all segmental peak systolic strain values within each territory. Details of the segmentation are given in figure 1. Longitudinal strain was computed based on the three apical planes and circumferential strain was based on the short-axis planes. The lowest absolute territorial strain value for each patient was assessed as a marker for identification of acute coronary occlusion. Correspondingly, territorial longitudinal and circumferential post-systolic shortening was calculated on a segmental basis as the difference between peak post-systolic strain and end-systolic strain. Peak systolic strain was defined as the maximum absolute value of peak negative strain (myocardial shortening) or peak positive strain (myocardial lengthening) during systole. The end of systole was defined by the aortic valve closure signal by Doppler flow.

The 16-segment left ventricular model. Territorial strain was calculated as average strain in segments belonging to the theoretical perfusion territory of each major coronary artery. The apical echocardiography planes are illustrated with dotted lines. The short-axis planes follow the basis to apex circles (mitral valve=segments 1–6, papillary muscle=segments 7–12, apex=segments 13–16). Modified after Cerqueira et al.18 2 Ch, two-chamber; 4 Ch, four-chamber; Aplax, apical long axis; CX, left circumflex artery; LAD, left anterior descending artery; RCA, right coronary artery.
Coronary angiography
All patients underwent coronary angiography, 27±18 h after admittance. Loops were digitally stored and interpreted by experienced operators. Acute coronary occlusion was defined as TIMI flow 0 or 1 in the infarct-related artery, based on lesion morphology and lack of collateral vessels. Intervention was performed when judged appropriate given angiographic, ECG and clinical data.
Contrast-enhanced MRI (ceMRI)
All patients with NSTEMI and no contraindications to magnetic resonance imaging (MRI) were invited to undergo a contrast-enhanced MRI (ceMRI) examination. Examinations were performed 8±4 months after admission, either with a 3 T scanner (Philips Achieva 3T, Philips Medical Systems, The Netherlands) or a 1.5 T scanner (Magnetom Sonata, Siemens, Germany). Late enhancement images were acquired 10–15 min after administration of a gadolinium-based contrast agent. No patient had evidence of coronary events between discharge and MRI. Total infarct size was reported as the percentage of LV muscle volume. Image analyses were performed using Segment version 1.8 (http://segment.heiberg.se (accessed 7 June 2010).19
Statistical analyses
The data were analysed using standard statistical software (SPSS version16.0). Continuous variables are presented as mean±SD or median (interquartile range). Differences between groups were analysed using Student t test, Mann–Whitney U test or one-way analysis of variance with Bonferroni correction applied for post hoc tests. Categorical variables are presented as numbers (%) and differences between groups were analysed by Fisher's exact test. Area under the curve, cut-off point, sensitivity and specificity for identification of acute coronary occlusions were determined by receiver operator characteristic (ROC) analysis. ROC curves were compared according to the method described by Hanley and McNeil,20 using dedicated statistical software (MedCalc version 10.4, Mariakerke, Belgium). Multiple logistic regression was performed to assess the potential benefit of combining the parameters studied in the ROC analyses. Changes in strain from coronary angiography to 3 months after discharge were tested with paired-samples Student t tests. Reproducibility of the echocardiographic analyses was calculated by intraclass correlation in 10 randomly selected patients. For all analyses, p values <0.05 were considered significant.
Results
Sixty-seven patients (61%) were diagnosed as NSTEMI, 18 (16%) as unstable angina and 26 (23%) as non-coronary chest pain. Baseline and clinical data for patients with and without acute coronary occlusion are given in tables 1 and 2. There were no differences in time from admittance to first echocardiographic examination, time from discharge to 3-month control or to MRI. At admittance, territorial circumferential and longitudinal strain, territorial circumferential and longitudinal post-systolic shortening, WMSI and CK-MB significantly differentiated patients with acute coronary occlusions from patients with non-occlusive disease. Clinical parameters, LVEF, ECG, TIMI or GRACE risk score did not differ significantly between the groups (table 2). There was a trend towards more frequent use of glycoprotein IIb/IIIa inhibitors in patients with acute occlusions. If patients with NSTEMI were assessed separately, this trend was reduced (33% vs 22%, p=0.37).
Patient characteristics according to whether or not the culprit lesion was an acute coronary occlusion.
Clinical, echocardiographic and angiographic findings, index hospitalisation
Echocardiographic parameters
Territorial circumferential strain demonstrated the best capability to identify acute coronary occlusions (figures 2 and 3, and table 3). In patients with acute occlusions, territorial circumferential strain was independently impaired regardless of culprit coronary perfusion area (left anterior descending artery (LAD): −6.6±1.0%; circumflex artery (CX): −6.3±2.9%; right coronary artery (RCA): −5.2±6.2; p=0.83). In a multiple regression model with territorial circumferential and longitudinal strain, territorial circumferential and longitudinal post-systolic shortening, WMSI, LVEF and CK-MB, only circumferential strain remained a significant predictor of acute occlusion.

Territorial strains in patients presenting with suspected non-ST-elevation acute coronary syndrome. Results are mean±SD.
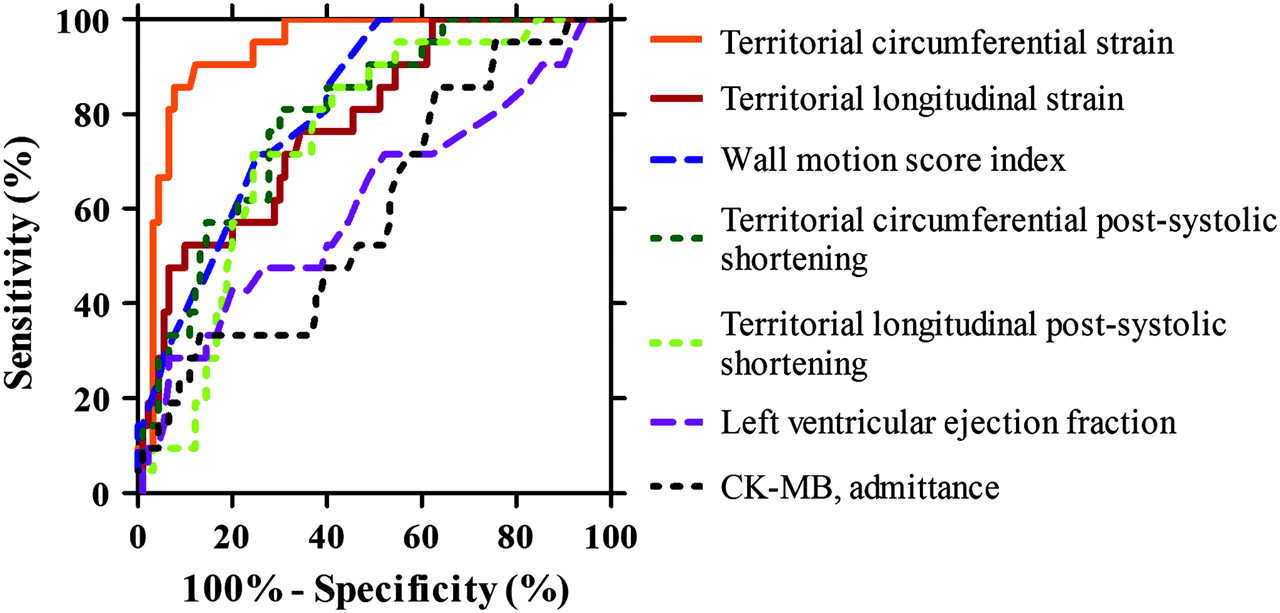
Early identification of acute coronary occlusions. Receiver operator characteristic analysis for detection of acute coronary occlusion in patients presenting with suspected non-ST-elevation acute coronary syndrome, including patients finally diagnosed as having non-coronary chest pain.
Identification of patients with non-ST-elevation acute coronary syndrome with acute coronary occlusions
Reproducibility was excellent for both territorial longitudinal and territorial circumferential strain. Intraclass correlations for intraobserver variability were 0.94 and 0.91, respectively, and for interobserver variability 0.92 and 0.83, respectively. Reproducibility was best in the LAD territory and lowest in the CX territory. Feasibility for strain measurements was excellent with 96.2% of the longitudinal and 93.0% of the circumferential segments analysed. All patients had satisfactory image quality for assessment of territorial strain. More segments were analysed in LAD and RCA territories than in the CX territory (97%, 97%, 89%, respectively, p<0.01).
Coronary angiography
Twenty-one of 67 patients (31%) with NSTEMI had an acute coronary occlusion at angiography. The culprit lesion was more frequently localised to the CX in patients with acute coronary occlusions than in those with non-occlusions, whereas no significant differences were observed between the groups for frequency of LAD or RCA culprit lesions (table 2).
Long-term myocardial function and infarct size
Long-term myocardial function and infarct size was evaluated in the 67 patients with NSTEMI. Sixty-four patients (96%) were examined by echocardiography and ceMRI was performed in 51 patients (76%). Twelve patients had contraindications to ceMRI and four were unable to comply. Figure 4 demonstrates more impaired LVEF in patients with acute occlusions than in patients with non-occlusive lesions (48±6% vs 57±6%, p<0.001). They also had more pronounced myocardial necrosis, as evident by peak troponin T (4.9±4.7 vs 0.9±1.1 μg/l, p<0.001) and infarct size by ceMRI (13±8% vs 3±3%, p<0.001). Except for angiotensin converting enzyme inhibitors and receptor blockers, which were more frequently used in patients with acute occlusions, there were no differences in drugs between the groups at follow-up.

Infarct size and long-term myocardial function in non-ST-elevation myocardial infarction (NSTEMI). Parameters for infarct size and long-term myocardial function in patients with NSTEMI, according to whether or not the infarct-related artery was occluded. Results are mean±SD. ceMRI, contrast-enhanced magnetic resonance imaging; LVEF, left ventricular ejection fraction.
Acute coronary occlusion was associated with larger infarct size than non-occlusion regardless of infarct-related artery (LAD: 13±8% vs 4±4%, p<0.01; CX: 16±10% vs 3±2%, p<0.01; RCA: 9±6% vs 2±1%, p<0.01). In patients with acute occlusions, there were no significant differences in infarct size or troponin T with regard to the territory of the infarct-related artery (p=0.44 and p=0.11, respectively). Patients with acute occlusions in the RCA had less impairment of LVEF than patients with acute occlusions in the CX (p<0.01).
Timing of coronary angiography was not a primary objective of this study. Thus, some patients underwent very early revascularisation, although they did not fulfil the criteria for urgent angiography. Six patients with NSTEMI due to acute coronary occlusions were revascularised within 12 h of symptom onset. These patients had a major improvement in longitudinal and circumferential myocardial function in the culprit territory after 3 months, whereas patients with acute coronary occlusions revascularised after more than 12 h had no improvement of function (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in strains according to timing of revascularisation in patients with non-ST-elevation myocardial infarction due to acute coronary occlusions. Longitudinal and circumferential territorial strains (mean±SEM) in the culprit territory according to whether percutaneous coronary intervention was performed within 12 h of symptom onset (n=6) or later (n=15). *p<0.01 for change from admittance to 3 months.
Discussion
This study is, to our knowledge, the first to demonstrate more impaired long-term LV function and larger infarct size in patients with NSTEMI due to acute coronary occlusions than in patients with NSTEMI and non-occlusive lesions. We introduce territorial circumferential strain by speckle-tracking echocardiography as a novel method for very early identification of acute coronary occlusions in patients with suspected NSTE-ACS, where clinical data, including risk score models, ECG and cardiac biomarkers fail to diagnose the occlusion.
Acute coronary occlusions in NSTE-ACS
Traditionally, NSTEMI and STEMI have been considered two different entities. This distinction, however, is based solely on the ECG, which has limited sensitivity to detect acute coronary occlusions.3 Both share the same pathophysiology, with quite similar risk factors, pathogenesis, complications and prognosis.5 Several trials have demonstrated comparable morbidity and mortality, even when corrected for age, treatment strategy and comorbidity.5 21 22
We found an infarct size in patients with NSTEMI and acute coronary occlusion that is comparable to that in the STEMI population,10 12 whereas most patients without acute occlusions had small infarcts. Both larger infarct size, higher levels of troponin T and impaired LV function are associated with poorer prognosis.23–25 Thus, our findings indicate that a distinction between NSTEMI with and without coronary occlusion may have important prognostic implications. This is also supported by a recent study by Wang et al, demonstrating higher risk-adjusted 6-month mortality in patients with NSTE-ACS due to occluded culprit vessels.2 Because irreversible myocardial injury may be avoided by urgent reperfusion, such distinction might also have implications for patient management in NSTE-ACS.
The majority of acute occlusions were localised to the CX. However, 43% were LAD or RCA occlusions. We demonstrated that the territory of the infarct-related artery did not affect infarct size. Thus, the importance of acute coronary occlusions in NSTE-ACS is not limited to the CX and the poor sensitivity of the ECG to identify occlusions in this territory.
Although few of the patients with NSTEMI and acute coronary occlusion underwent very early revascularisation (within 12 h), improvement of myocardial function strongly indicates a benefit with urgent revascularisation in this subgroup of patients.
Identification of acute coronary occlusion in NSTE-ACS
In STEMI, reperfusion has to be performed within 12 h, and preferably within 2 h, to avoid irreversible myocardial injury.26 If this applies to patients with NSTE-ACS due to acute coronary occlusions, these patients need to be identified very early. At admittance, clinical parameters, ECG or cardiac biomarkers could not precisely identify patients with acute occlusions. Although there were non-significant trends in GRACE score and recurrent angina, our findings demonstrate that current methods for risk evaluation are inadequate to identify acute coronary occlusions at hospitalisation. The borderline difference in use of glycoprotein IIb/IIIa inhibitors was primarily driven by troponin T positivity.
Echocardiography is easily accessible in the acute setting of NSTE-ACS. It has previously been reported that strain by echocardiography is better than wall thickening in discriminating infarct from non-infarcted myocardium,27 and that strain by echocardiography and by MRI differentiates transmural from non-transmural infarction, with circumferential strain better than longitudinal strain.8 12 28 However, there are no published data on the ability to detect acute coronary occlusions in the setting of NSTE-ACS. We demonstrated that territorial circumferential strain was better than territorial longitudinal strain, WMSI, post-systolic shortening and LVEF in this population. We chose not to analyse radial strain, as it has methodological limitations and has been shown to be inferior to circumferential and longitudinal strain in identifying ischaemia and necrosis.8 11
The superiority of circumferential strain over longitudinal strain is probably due to the helical structure of myocardial fibres, with subendocardial fibres having a dominant longitudinal direction, whereas mid-myocardial fibres are more circumferentially oriented.29 With increasing severity, ischaemia and necrosis propagate in a transmural wavefront extending from the endocardium to the epicardium.30 Thus, our finding may represent different degrees of transmural ischaemia. Non-occlusive coronary lesions probably cause predominantly subendocardial ischaemia with impaired longitudinal function. In contrast, acute coronary occlusions cause transmural ischaemia with both longitudinal and circumferential dysfunction (figure 3). This is also evident from the finding of a small infarct size in patients with non-occlusive lesions. Even though a higher number of longitudinal segments were analysed by strain compared with circumferential segments, the latter performed better in the diagnosis of acute coronary occlusions. Therefore, any possible difference in image quality is not expected to have influenced the results.
Given the potentially substantial myocardial injury with coronary occlusions, a feasible method for identification should have very high sensitivity. In this population, the cut-off value for territorial circumferential strain resulted in only two patients with false-negative results (lesions localised to the middle part of the CX and middle part of the RCA, infarct size 10% and 9%, respectively). Five of six patients missed by WMSI were correctly diagnosed by territorial circumferential strain. Conversely, among 11 patients falsely identified as having an acute occlusion using the cut-off value for territorial circumferential strain, 10 had high-grade coronary stenoses with TIMI-flow >1. They constitute a group of patients likely to be at increased risk who would potentially benefit from early revascularisation. The severe depression of myocardial function in these patients may have been due to severe ischaemia and stunning. Because patients received quite extensive antithrombotic and anticoagulant treatment, it is also possible that some lesions which were occluded at admittance underwent partial lysis while awaiting coronary angiography.
Clinical perspective
These findings suggest that more attention should be given to acute coronary occlusions in NSTE-ACS. The potential benefit of acute revascularisation needs to be assessed in randomised clinical trials. If such studies were performed, accurate methods would be needed for the early risk stratification. We demonstrated that territorial circumferential strain has excellent ability to identify coronary occlusions in the acute setting of NSTE-ACS, and has the potential to become such a method.
Limitations
An important limitation of this study is the lack of long-term clinical end points. Such results were, however, recently reported by Wang et al2 and in accordance with our findings.
The described method for assessment of coronary territories does not take into account individual variations in coronary anatomy or the size of the area at risk, and some overlap between the area at risk and non-ischaemic myocardium is expected. This model, however, is feasible because it does not require other information about the culprit area.
Only standard ECGs were routinely obtained, thus any benefit of posterior ECG leads could not be assessed. Similarly, contrast perfusion echocardiography is evolving as a feasible technique for assessment of myocardial perfusion and might improve the precision of identification of acute coronary occlusion.
This study only assessed patients without a history of myocardial infarction and the results could not routinely be generalised to patients with depressed myocardial function due to scar or cardiomyopathies. Identification of acute coronary occlusions in this setting needs to be assessed in a separate study. However, if previous echocardiographic examinations have demonstrated well-preserved myocardial function, a severe impairment of territorial circumferential strain is likely to be related to the present event.
Conclusions
Acute coronary occlusion is a common finding at coronary angiography in patients with NSTEMI. We demonstrated that patients with acute occlusions develop larger infarcts and more impaired LV function than patients with NSTEMI without occlusions, regardless of infarct-related artery. Territorial circumferential strain by echocardiography enables very early identification of acute coronary occlusions in patients with NSTE-ACS and may be used for detection of patients who urgently need revascularisation.
References
Footnotes
Funding The study was supported by the South-Eastern Norway Regional Health Authority, the Norwegian Foundation for Health and Rehabilitation and Sørlandet Hospital HF. The supporters of the study had no role in the study design, collection, analyses or interpretation of data, or writing of the manuscript.
Competing interests None.
Ethics approval This study was conducted with the approval of the Southern Norway Regional Committee for Medical Research and Ethics.
Provenance and peer review Not commissioned; externally peer reviewed.