Article Text

Abstract
Objective: To identify clinical markers available within the first 48 hours of admission that are associated with poor outcome in infective endocarditis.
Designs: Retrospective cohort study.
Setting: Teaching hospital.
Patients: 208 of 220 patients with infective endocarditis.
Methods: Consecutive patients with infective endocarditis presenting between 1981 and 1999 to a tertiary centre were studied. Clinical, echocardiographic, and haematological data recorded within 48 hours of admission were obtained. Data were analysed using logistic regression models.
Main outcomes measures: Mortality at discharge and at six months.
Results: Data were obtained for 93% of patients who were eligible for inclusion. 194 (93%) were positive for Duke criteria. Mean age was 52 (1.2) years, and 138 (66%) were men. 82 (39%) were transferred from other hospitals. 181 (87%) were blood culture positive, and 47 (23%) infections were Staphylococcus aureus. The infection was located on aortic (n = 85, 41%), mitral (n = 77, 37%), tricuspid (n = 18, 9%), and multiple valves (n = 20, 10%). 67 (32%) had prosthetic valve endocarditis. 48% of the cohort were managed with antibiotics alone. Mortality at discharge was 18% and at six months 27%. Duration of illness before admission, age, sex, valve infected, infecting organism, and left ventricular function were not predictors of adverse mortality. However, abnormal white cell count, serum albumin concentration, serum creatinine concentration, or cardiac rhythm, the presence of two major Duke criteria, or visible vegetation conferred a poor prognosis.
Conclusions: Conventional prognostic factors in this study did not appear to predict outcome early during hospital admission. However, simple clinical indices, which are readily available, are reliable, cheap, and potentially powerful predictors of poor outcome.
- infective endocarditis
- mortality
- outcome
- prognostic factors
- CRP, C reactive protein
- ESR, erythrocyte sedimentation rate
- UCLH, University College London Hospitals
- WCC, white cell count
Statistics from Altmetric.com
- CRP, C reactive protein
- ESR, erythrocyte sedimentation rate
- UCLH, University College London Hospitals
- WCC, white cell count
Microbial infection of the endothelial surface of the heart, or infective endocarditis, remains a challenging disease to manage. Initial diagnosis may be difficult to establish and antimicrobial and surgical strategies for treatment need to be carefully administered.1 Despite the major advances in diagnostic technology and improvements in antimicrobial selection and monitoring, accompanied by parallel advances in surgical techniques, the morbidity and mortality remain high: one in five patients die during the initial hospital admission.2,3 There are several possible explanations for this continuing high mortality including changes in the type and virulence of infecting organisms and changes in the population at risk of developing infective endocarditis. However, clinicians are hampered by the inability to predict accurately the course of disease and its short and long term prognoses.
Several retrospective studies have defined clinical and laboratory findings that may have prognostic importance. However, none of these specifically studied those features that can influence outcome early in the course of the disease. Many of these studies have looked at the importance of recognised specific factors2,4 or, in more recent studies, examined the influence of conventional high risk predictors at any time during the admission.
Prompt identification of patients with a high risk of death or of developing complications or who are likely to need a prolonged hospital admission is important. The ability to identify such patients may modify management strategies, particularly regarding transfer to regional centres.5–7 The aim of our study was to identify clinical and laboratory findings present within 48 hours of admission that had an influence on short and longer term outcomes. Short term outcomes were defined as in-hospital mortality and longer term outcomes as mortality at six months following discharge from hospital.
METHODS
The University College London Hospitals (UCLH) ethics committee approved this study. We performed a systematic retrospective case notes review and questionnaire survey of patients admitted with a diagnosis of infective endocarditis to UCLH between 1981 and 1999. Our hospital is a tertiary referral centre, which receives patients with infective endocarditis from surrounding hospitals, in addition to those that arise within our own catchment area.
At our institution the microbiologists are involved in the management of all cases treated as infective endocarditis. Cases could therefore be identified from a clinical database held in the microbiology department. The microbiology data were recorded prospectively. The data were the patient's name and age, pathogen and date of isolation, number of positive cultures, antibiotic susceptibilities, minimum inhibitory concentration if determined, and records of daily visits including antibiotic usage and clinical progress. The information was consistent throughout the study period and for 12 years was recorded by a single observer. From the list of patients we obtained data on baseline demographic features and a range of clinical and laboratory findings that we wished to assess as potentially important in predicting outcome. Data were collected on all patients within 48 hours of their “original” admission whether they came from a referring hospital or not. Patients transferred from a referring hospital usually came with a detailed doctor's letter, which included blood results on admission. If data were not available, we visited the referring hospital to establish these results. Where there was more than one result, the earliest available result was used. Even where the diagnosis of infective endocarditis was established later into the admission, data available within the first 48 hours of admission were used for analysis. When this information was not available in the medical notes, postal and telephone questionnaires, addressed to both the patients and their general practitioners, were used.
Data were missing for several reasons. Firstly, notes that are nearly 20 years old do not keep very well and a lot of important facts can be misplaced. Many blood results are not filed appropriately and are lost in transit. Secondly, if blood results were not documented in the notes, then missing data were identified in a visit to the biochemistry and haematology laboratories. If they were not found it was assumed that the certain blood tests were not requested.
The following data were recorded:
Baseline demographics: age (< 65 or > 65 years), sex, date of admission, duration of illness before hospital admission, origin of patient (referred hospital or UCLH patient), and number of days with referring hospital.
Clinical findings: body mass index, comorbid conditions (such as diabetes, ischaemic heart disease, hypertension, cerebrovascular event, and congenital heart disease), factors predisposing to infective endocarditis (rheumatic fever, misuse of infected drugs, central line within previous six months), and possible sources of infections (such as a recent dental treatment, skin lesions, or recent invasive procedure).
Abnormal haematological findings: serum creatinine concentration > 133 μmol/l (this being the upper limit for creatinine derived from the hospital database), serum albumin concentration < 30 g/l, white cell count (WCC) < 3 × 109/l or > 11 × 109/l, C reactive protein (CRP) concentration > 100 mg/l, and erythrocyte sedimentation rate (ESR) > 7 mm/h (for those < 40 years of age) and > 20 mm/h (> 40 years of age).
Findings on ECG: abnormal cardiac rhythm, defined if there was any other rhythm than sinus or sinus tachycardia (heart rate > 100 beats/min).
Findings on echocardiography: location of visible vegetation, type of valve infected, impaired left ventricular function, valve regurgitation. All echocardiograms were transthoracic but since 1994 the vast majority of patients had an additional transoesophageal echocardiogram. This was not differentiated for the purpose of the study, as it was not always clear from the notes what type of was made.
Microbiological data: blood culture status and type of organism, antibiotic treatment, and duration of antibiotic treatment. Recurrent infective endocarditis was defined as a second episode of infective endocarditis within six months of the first episode with a similar organism. Reinfection was defined as second episode of infective endocarditis with another organism. Cases of culture negative endocarditis excluded those in which the cause was identified by culture of valve tissue or serology.
Furthermore, we assessed whether these cases conformed to a previously conventional diagnostic classification system (Duke criteria) proposed by Durack and colleagues8 and whether this influenced prognosis.9 The need for surgical intervention was also assessed.
Outcome measures analysed were in-hospital mortality and mortality at six months.
Statistical methods
The influences of categorical risk factors on both mortality outcomes were initially assessed using either χ2 tests or, where appropriate, Fisher's exact test. To test whether the mean of each normally distributed continuous risk factor was similar in those who died and those who did not, t tests were used. The odds ratio and its 95% confidence interval were also calculated for each factor in relation to both in-hospital and six month mortality. Risk factors that exhibited an important association with the outcomes of interest in these unadjusted analyses were considered for inclusion in multiple regression modelling. Multiple logistic regression was used to determine the independent risk factors for mortality at discharge and mortality up to six months. All analyses were carried out using SPSS 8.0 (SPSS Inc, Chicago, Illinois, USA) and Prism 3.0 (GraphPad Software, San Diego, California, USA).
RESULTS
Two hundred and twenty patients were identified from the database held within the microbiology department as being treated for infective endocarditis between 1981 and 1999. We were able to collect comprehensive data on 208 of them. Twelve patients were not included because their medical notes were missing. Sketchy data were deemed inappropriate for inclusion in the cohort.
Demographics
The mean age of the cohort was 52 (1.2) years, 66% (n = 138) were men (mean age 51 (1.4) years), and 34% (n = 70) were women (mean age 54 (2.1) years). Overall mortality at discharge was 18% (n = 38) and at six months this increased to 27% (fig 1). There was a major increase in the number of cases treated as infective endocarditis between the decades 1981–1990 and 1991–1999 (n = 49 v n = 159) but there was no significant difference in mortality between these groups (fig 2).

Comparison between in-hospital and six month mortality.

In-hospital and six month mortality analysed by decades.
Sex and age
Sex or age was not a factor that affected mortality at discharge or six months (tables 1 and 2). The median duration of illness before admission was 21 days (range 0–240).
Factors associated with in-hospital mortality: unadjusted estimates
Factors determining six month mortality: unadjusted estimates
Duration of illness before admission
The median duration of illness before admission for patients who died in hospital was 20 days (range 1–90 days) compared with 41 days (range 0–240 days) for those who survived this period (p < 0.05). Mean length of hospital stay was 50 (2.1) days. Of those admitted directly to our hospital infective endocarditis was the admitting diagnosis in 64% (n = 81) and in the remaining 34% the diagnosis was made after hospital admission.
Origin of patients
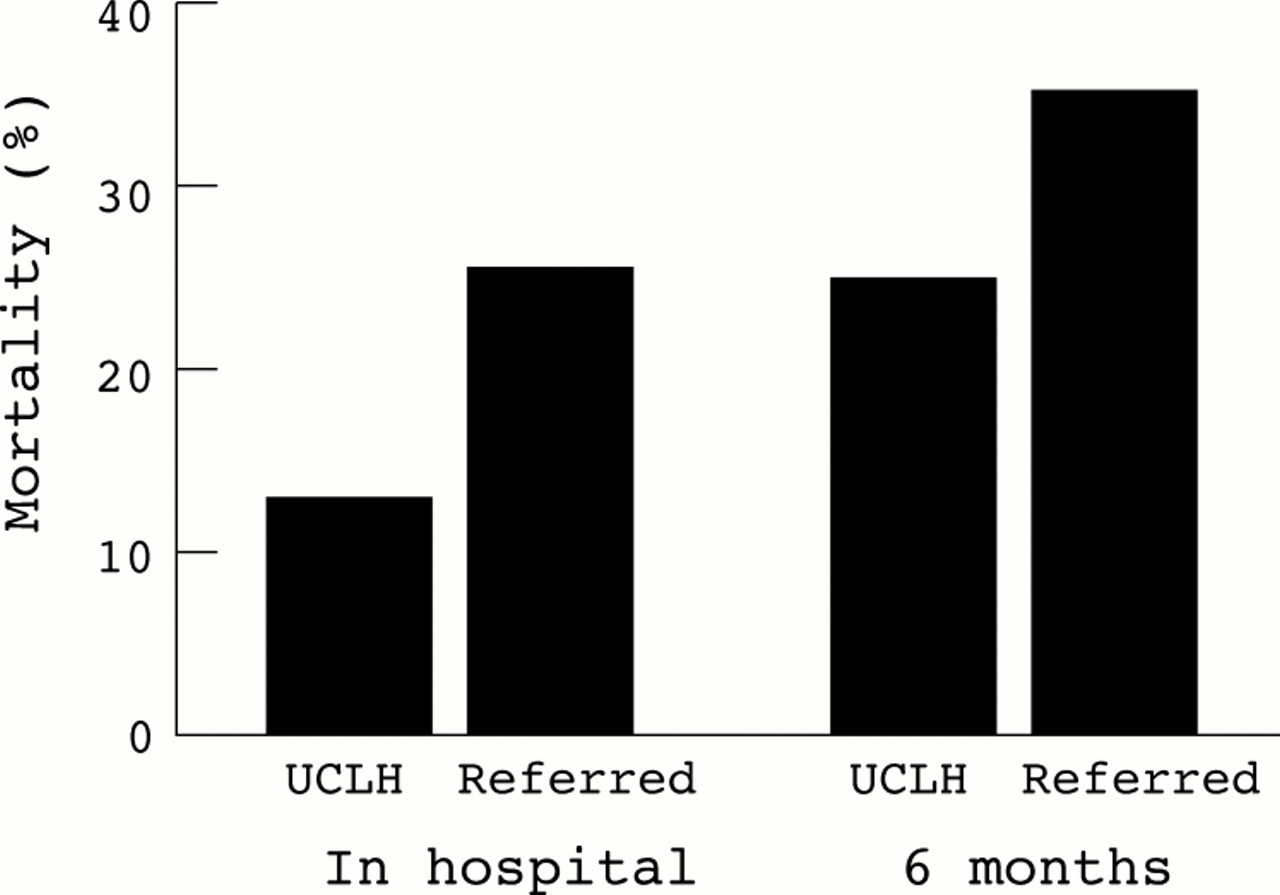
Of the 208 patients, 82 (39%) were transferred from another hospital. In-hospital mortality in this group was 21 (26%) compared with 16 (13%) in those admitted directly (p = 0.03) (table 1, fig 3). At six months this difference remained significant: 26 (35%) in the referred group compared with 22 (20%) of those admitted directly (table 2, fig 3). There were no differences in basic demographic factors between patients who were admitted from a referring hospital or through our hospital. However, 60 (73%) of those referred from other hospitals proceeded surgery whereas only 40 (32%) of UCLH patients required surgery.

{kind=link}
{kind=link}
{kind=link}
Comparison between in-hospital and six month mortality in patients admitted directly to University College London Hospitals (UCLH) and referred patients.
Clinical findings
Diabetes
Mortality in the diabetic group (n = 14) at discharge was 5 (36%) compared with 30 (16%) in the non-diabetic group (table 1). This difference did not reach conventional significance levels (p = 0.07), although the numbers of patients with diabetes in the study were small. By six months the comparable figures were 6 (43%) and 41 (25%) (p = 0.1; table 2). Other comorbid illnesses did not confer a poorer prognosis although numbers were small (tables 1 and 2).
Predisposition
Table 3 shows the breakdown of predisposing and non-predisposing factors in 183 (88%) patients. The presence versus absence of a predisposing factor was associated with lower in-hospital (16% v 33%) and six month mortality (24% v 48%) (tables 1 and 2).
Predisposing factors
Body mass index
Admission weight or body mass index had no influence on outcome (tables 1 and 2).
There were 19 (9%) users of injected drugs in the population. They were young (mean age 32 (1.4) years). There was an excess of tricuspid valve involvement in this group (58% v 7%) but mortality was not affected.
Haematological findings
Creatinine
Creatinine was measured in 196 (94%) patients and was strongly associated with mortality. Patients with abnormal creatinine had a mortality rate of 17 (30%) at discharge compared with 19 (14%) in-patients with normal renal function (p = 0.01; table 1). Longer term prognosis was also influenced at six months with a mortality rate of 20 (39%) in the group with an increased creatinine, compared with 28 (22%) in those with normal creatinine concentrations (p = 0.02; table 2).
Serum albumin
Serum albumin was measured in 192 (92%) patients in the first 48 hours of admission. Those with an abnormal serum albumin concentrations (n = 59) had a significantly higher mortality rate (36%) than those with a normal serum albumin (9%). This difference was also observed at six months (p = 0.0007).
White cell count
WCC was documented in 192 (92%) patients within 48 hours of admission. WCC was strongly associated with mortality. Patients with WCC outside the normal range were at a significantly greater risk of death at both discharge and six months. In patients who had an abnormal WCC (n = 90) there was a 32% compared with 4% (p < 0.0001) in-hospital mortality rate in those with a normal WCC, which increased to 41% compared with 12% at six months (p < 0.0001; tables 1 and 2).
C reactive protein
CRP was measured in only 129 (62%) patients. Mortality was not affected in patients with an abnormal CRP concentration at either discharge or six months (tables 1 and 2). The mean CRP concentration of patients who died in hospital was significantly higher than in those who survived (167 (28) v 99 (9) mg/l, p < 0.05).
Erythrocyte sedimentation rate
ESR was measured in 144 (70%) subjects within 48 hours of admission. There was greater in-hospital mortality among patients with normal ESR than among those with an abnormal ESR (28% v 13%; table 1), although this did not reach significance. A similar trend was also observed at six months (40% v 21%; table 2). Using a cut off of ESR of 50 or 100 mm/h, or considering ESR as a continuous variable, did not affect this result.
ECG and echocardiographic data
Heart rhythm
ECG was recorded at admission in 190 (91%) patients. Cardiac rhythm was abnormal in 82 (43%) patients and 19 (23%) of these patients had died by discharge (table 1). The difference was most pronounced at six months: mortality was 26 (35%) in those with an abnormal rhythm compared with 16 (16%) in those with normal rhythm (table 2).
Valve type
In 141 (67%) patients there was an infection of native valves. Their mean age was 50 (1.4) years. Patients with prosthetic valve endocarditis (n = 67) were older (mean age 56 (1.8) years, p ≤ 0.05). Prosthetic valve endocarditis did not affect mortality (table 1); however, it did fail marginally to reach significance at six months (table 2).
Visible vegetation
During the initial 48 hours of admission, 137 (66%) patients underwent either transthoracic or transoesophageal echocardiography. There was a visible vegetation in 128 (62%) and although this did not significantly influence in-hospital mortality (22% v 13%; table 1) it did influence six month mortality (32% v 19%; table 2).
Left ventricular function and valve regurgitation
Patients with poor left ventricular function defined by echocardiography (n = 17) did not have an increased mortality at either discharge or six months (tables 1 and 2). The presence of severe regurgitation on either aortic or mitral valve was associated with increased mortality in hospital and at six months (26% and 37%, respectively) compared with those without severe regurgitation (12% and 18%, p < 0.05 for both; tables 1 and 2).
Embolic event
The presence of an embolic event within 48 hours of admission was documented in 38 patients. There were 21 cerebrovascular events, 5 pulmonary emboli, and 9 peripheral arterial emboli. These had no influence on outcome (tables 1 and 2). The presence of a visible vegetation or atrial fibrillation did not increase the risk of an embolic phenomenon.
Valve infected
Aortic valve infective endocarditis was the most common type; valves affected were aortic in 85 (41%), mitral in 77 (37%), and tricuspid in 18 (9%). Aortic or mitral location of infective endocarditis did not influence mortality. Multiple valve involvement conferred a high mortality both in hospital and at six months (table 4), although numbers in the different groups are too small to carry out statistical testing.
Distribution of valve infected and mortality
Microbiological findings
Blood culture status
Blood cultures were positive in 181 (87%) cases. α Haemolytic streptococci (n = 53, 29%) were the most common pathogens isolated, followed by Staphylococcus aureus in 47 (26%), and enterococci in 23 (13%; table 5). There was no difference in the mortality in hospital or at six months between culture positive and culture negative patients (in-hospital mortality: 35 (19%) v 3 (11%), respectively; six month mortality: 44 (27%) v 6 (23%), respectively; tables 1 and 2).
Distribution of infecting organisms and mortality
Staphylococcus aureus
Neither S aureus nor culture negative endocarditis conferred a worse prognosis than other types (tables 1, 2, and 5). Patients with S aureus endocarditis presented to hospital earlier than those with infection by other organisms (13 days v 46 days, p < 0.05). Methicillin resistant S aureus was found in one patient. Of the 47 patients infected with S aureus 12 (25.5%) had tricuspid valve involvement and of these, 10 were users of injected drugs and none of them died.
Nineteen patients had recurrent infective endocarditis and five had a reinfection during this period. Neither reoccurrence nor reinfection affected any feature of outcome, as the numbers were too small.
Duke criteria
The “definite” diagnostic criteria of the Duke criteria classification (two major, one major/three minor or five minor) were fulfilled by 194 (93%) patients, although it did not predict outcome. However, having two major criteria compared with any of the other combinations was associated with a higher mortality at six months (32% v 19%, p = 0.04; tables 1 and 2).
Surgery
Surgery was performed in 107 (51%) patients. In-hospital mortality was not influenced by surgery (22% v 15% in the non-surgical group; table 1). At six months there was a trend towards increased mortality in the surgical group (33% v 20%; table 2).
Multiple regression models
A multiple logistic regression model found that WCC and serum albumin were independent indictors of mortality, both at discharge and at six months' follow up. No other factors were independently associated with mortality at discharge, while heart rhythm was associated with outcome at six months. WCC was strongly associated with outcome and was responsible for reducing the effect of the other indicators, which had been associated with outcome in the unadjusted analyses. The adjusted odds ratio for WCC in relation to mortality at discharge was 8.58 (95% confidence interval (CI) 2.77 to 26.52, p = 0.0002) and that for mortality at six months was 3.66 (95% CI 1.58 to 8.45, p = 0.002). The odds ratios for serum albumin from the adjusted models were 4.80 (95% CI 1.96 to 11.74, p = 0.0006) for outcome at discharge and 3.07 (95% CI 1.36 to 6.94, p = 0.007) at six months. The odds ratio for heart rhythm at six months was 2.32 (95% CI 1.04 to 5.15, p = 0.04). These results remained after further adjustment for the potential confounders of age and sex. The possibility that having diabetes is an independent risk factor for mortality was also observed. The estimated odds ratios observed in the unadjusted analyses were hardly attenuated when added to the models described above, but the small number of patients with diabetes means there is a lack of power to be able to detect a significant difference.
DISCUSSION
The novel and clinically important observations from this study are that simple and readily available clinical and laboratory findings available with 48 hours of admission are strongly associated with in-hospital and six month mortality in patients treated for infective endocarditis. An abnormal (either increased or decreased) WCC and abnormal albumin concentration were independently associated with in-hospital mortality and conferred a ninefold and threefold increased odds of dying during the admission. These factors also predicted six month mortality. An abnormal heart rhythm on admission was an independent predictor of six month mortality.
The measures of inflammation reflect the systemic response to infection and suggest that infective endocarditis should be viewed as a systemic sepsis. Many scoring systems are used to predict outcome in various states of sepsis and in many such models WCC and albumin are important variables.10,11 To our knowledge our study is the first to confirm that these markers are independent predictors of mortality in the setting of infective endocarditis. In addition we showed that the mean CRP concentration of patients who died during hospital admission was significantly higher than that of those who survived. This has also been reported by others.3 CRP is an acute phase protein produced by the liver and is used in a number of studies to quantify the inflammatory response. The use of CRP to monitor infective endocarditis may be preferred to using ESR.12 Although an increased ESR is classically associated with infective endocarditis our data suggest that a normal ESR may suggest a poorer outcome.13 Though this failed to reach significance (p = 0.07), the differences in mortality between patients with a normal and those with an abnormal ESR suggest that those who fail to mount a suitable response early in the course of the disease are a higher risk group. A very small population of patients had an ESR determined within 48 hours of admission but some of these patients were admitted under another physician and not a cardiologist. An ESR result may not have been seen as appropriate at that time. The measurement of ESR is confounded by the degree of anaemia. We did not collect information about anaemia but it would be valuable to address this in future studies. Our data suggest that clinicians should be wary of excluding a diagnosis of infective endocarditis with a normal ESR if the clinical picture suggests that diagnosis and that CRP is a better test in this setting.
Abnormal serum creatinine on admission was associated with increased mortality. There are several reasons for renal function to be impaired in infective endocarditis, including immune complex mediated glomerulonephritis, renal artery embolism, antibiotic toxicity, and haemodynamic disturbance.14 We could not ascribe this association to a more prolonged illness leading to renal impairment and it is likely that renal dysfunction again reflects a systemic manifestation of infective endocarditis. Other studies have defined the importance of renal failure (defined by a creatinine concentration > 180 μmol/l) in predicting prognosis but our data suggest that even a mildly abnormal creatinine concentration on admission carries a poor prognosis.15,16
Sex and age did not influence outcome in our cohort although some groups have suggested that age may be important.17 Age and sex did account for relations observed between WCC, serum albumin, and outcome, although mortality was higher in older and in female patients. Patients who have a longer duration of illness before hospital admission do better and this may reflect the indolent course of their disease. Those who have more aggressive disease with more symptoms are likely to seek medical attention earlier. Staphylococcal endocarditis is classically associated with a more florid presentation and in fact the mean duration of illness before admission for those with staphylococcal infection was shorter than for those with other organisms.
The majority of patients were blood culture positive and we confirmed that blood culture status does not itself influence prognosis.18 Previous reports have suggested that enterococci, S aureus, and non-viridans streptococci carry a poorer prognosis but this is not supported by our data. It is important to note that among the patients with S aureus infection there was high incidence of tricuspid valve involvement in which no deaths occurred, possibly accounting for this unconventional finding.
Patients who were referred from other hospitals had a higher in-hospital and six month mortality. We could not identify any obvious features that would explain this trend but this may reflect case selection in that many more of these patients went on to have surgery.9 In our series surgery itself did not influence survival in the whole cohort, although there was a non-significant trend towards increased mortality in the surgical group at six months' follow up.
In our series the number of patients with diabetes was small but they had a high inpatient mortality. This trend to increased mortality suggests that future studies should address the impact of this condition on the nature of infective endocarditis. An intriguing observation was that patients identified as having a predisposition to infective endocarditis did significantly better than those without. Although we could not define any obvious explanation for this it is possible that physicians involved in the management of such patients would have a heightened awareness to the possibility of infective endocarditis in this group.
We were unable to define any influence of the site of infective endocarditis or valve type on prognosis, but multiple valve involvement clearly carries an adverse prognosis. Echocardiographic findings that influence prognosis are visible vegetations, which influence six month mortality, and the presence of severe regurgitation on left sided valves, which influenced both in-hospital and six month mortality. Surprisingly, documented poor left ventricular function did not influence prognosis.
The Duke classification is now an established diagnostic clinical scheme for infective endocarditis. We showed that the combination of two major criteria is associated with a more invasive form of the disease at six months' follow up.
In our series we were unable to show an influence of age, surgery, prosthetic valve or aortic valve endocarditis, or specific organism on outcome, which have previously been associated with high mortality. This may be related to the changing spectrum of antibiotics and advances in surgical techniques, since many of these reports were published in the early 1990s, and the nature of the disease and management have been developed over the past decade.19
Our data also highlight that there were further deaths in patients in the first six months following an admission for infective endocarditis. This important point has not been addressed in studies looking at longer term prognosis. The survival curves in these studies show an early attrition that has not been systematically assessed. Our data suggest that in the immediate convalescent period patients should be aggressively monitored and practitioners involved in the management of these patients should be alerted to seeking early specialist opinions if there are any complications.
In summary, this study has shown that patients with infective endocarditis who have an abnormal WCC, serum albumin concentration, heart rhythm and rate, serum creatinine concentration, the presence of two major Duke criteria, or a visible vegetation at initial echocardiography carry a poorer prognosis. Identification of these features should prompt consideration of early transfer to the regional surgical centre. Although there is no evidence that early surgical intervention would necessarily improve outcome in these patients, regional centres are able to respond to developing complications more quickly. Infective endocarditis remains a complex disease and these data provide insight into the importance of recognising the systemic nature of the disease and being mindful that simple clinical and laboratory findings remain powerful tools that may guide the management of these challenging patients.