Article Text

Abstract
Cardiac contusion is usually caused by blunt chest trauma and therefore is frequently suspected in patients involved in car or motorcycle accidents. The diagnosis of a myocardial contusion is difficult because of non-specific symptoms and the lack of an ideal test to detect myocardial damage. Cardiac contusion can cause life threatening arrhythmias and cardiac failure. Many diagnostic methods, such as ECG, biochemical cardiac markers, transthoracic and transoesophageal echocardiography, and radionuclide imaging studies, have been investigated to determine their use in predicting such complications. Recently, cardiac troponin I and T were found to be highly sensitive for myocardial injury. Troponin I and T have also proved to be useful in the stratification of patients at risk for complications. Nevertheless, diagnosis of a cardiac contusion and identification of patients at risk remain a challenge. In this review the current diagnostic tests will be discussed. Also, based on these diagnostic tests, a screening strategy containing data from the latest studies is presented, with the intention of detecting patients at risk.
- cardiac contusion
- blunt chest trauma
- diagnostic protocol
- CK, creatine kinase
- CK-MB, cardiospecific MB isoenzyme of creatine kinase
- TOE, transoesophageal echocardiography
- SPECT, single photon emission computed tomography
Statistics from Altmetric.com
- CK, creatine kinase
- CK-MB, cardiospecific MB isoenzyme of creatine kinase
- TOE, transoesophageal echocardiography
- SPECT, single photon emission computed tomography
The exact incidence of a cardiac contusion in patients with blunt chest trauma is unknown. The reported incidence ranges between 3–56% of patients, depending on the criteria used for establishing the diagnosis. High incidences of cardiac injury, varying between 29% and 56%, were found in ECG studies.1–5 In studies of the cardiospecific MB isoenzyme of creatine kinase (CK-MB), incidences of approximately 19% were found.1,6 Echocardiographic evidence of myocardial injury was detected in 3–26% of patients using a transthoracic approach1–3,7–9 and in 27–56% of the patients using a transoesophageal approach.9–12 Recent studies that used the highly specific cardiac markers troponin I or T for the diagnosis of a cardiac contusion reported incidences ranging between 15–24%.5,7,8 Therefore, a substantial number of patients with blunt chest trauma are suspected of having cardiac injury.
Possible complications of cardiac injury, such as life threatening ventricular arrhythmias and cardiac failure, are less common and were described in up to 16% of patients.1–3,9,13,14 If patients receive adequate treatment for such complications, death due to cardiac causes is rare. In one study, one patient (1.5%) died of persistent cardiogenic shock and in another study three severely injured patients died before treatment had been started.2,8
In mildly injured patients a cardiac contusion is generally well tolerated. The majority of such patients never suffer any symptoms and proceed to an uncomplicated recovery with an excellent prognosis. However, life threatening ventricular arrhythmias and cardiac failure can also occur in these symptomless patients. It is therefore important to screen all patients with blunt chest trauma to identify those at risk for complications.
CAUSES AND CLINICAL FEATURES OF BLUNT CHEST TRAUMA
Blunt cardiac injury is most frequently caused by road traffic accidents and results from a direct blow to the chest from a steering wheel or rapid deceleration.2,6,13 A direct blow to the precordium or a sustained force to the thoracic wall compresses the heart between the sternum and spine. In rapid deceleration accidents the heart, which has relatively free movement in the anteroposterior direction, continues to move forward due to its momentum and strikes the internal sternum with considerable force. Other less frequent causes are falls from a great height, sport injuries, blast forces, and indirect compression on the abdomen with upward displacement of abdominal viscera.13,15
Cardiac contusion clinically presents as a spectrum of injuries of varying severity.6,13,16 Patients with severe myocardial injury are easily detected in case of haemodynamic instability. However, cardiac symptoms such as hypotension or hypoxia can be easily masked in trauma patients due to other severe injuries with blood loss or associated pulmonary, vascular, and neurological injuries. The diagnosis of cardiac contusion in trauma patients without evident clinical signs of myocardial injury is more difficult. Myocardial contusion may produce only mild symptoms, such as palpitations or precordial pain, which is often attributed to concomitant musculoskeletal injury.4 Although the majority of patients with blunt chest trauma have chest wall lesions, absence of thoracic lesions decreases the suspicion but never excludes cardiac injury.15,17 Chest radiography and thoracic computed tomography provide no additional information for the diagnosis of cardiac contusion but may show associated injury of the great vessels, or skeletal or pulmonary structures.18–20 The role of magnetic resonance imaging in the detection of acute myocardial injury has not yet been established.18 However, for the evaluation of the spine, diaphragm, and thoracic aorta in haemodynamically stable patients with blunt chest trauma, magnetic resonance imaging has been described as an accurate alternative to computed tomography, in case of suboptimal images.18,21
BIOCHEMICAL CARDIAC MARKERS
A cardiac contusion is histologically characterised by intramyocardial haemorrhage, oedema, and necrosis of myocardial muscle cells. These histological findings are almost similar to those seen in acute myocardial infarction.13,22 Therefore, cardiac enzyme determinations were the first screening tool used to detect myocardial injury. Creatine kinase (CK) is non-specifically increased in trauma patients caused by associated skeletal muscle injury. CK-MB is known to have a better specificity in acute myocardial infarction. However, in multitrauma with high CK concentrations many false positive increases were found.6,13 The usefulness of CK-MB determination seemed to be restricted to the detection of myocardial trauma in case of mild non-cardiac injuries.23 More recent studies reported low sensitivity and specificity of CK-MB for cardiac injury in this category of mildly injured patients.3,14,24,25 Therefore, CK-MB determination is of limited value in the detection of myocardial injury.
Serum cardiac troponins, troponin I and troponin T, are highly specific to myocardial injury. They are myocardial regulatory contractile proteins not found in skeletal muscles and are released into the circulation only after loss of membrane integrity. The latest studies showed high accuracy of both troponin I and troponin T in the diagnosis of cardiac injury.7,8 Moreover, a normal concentration of cardiac troponin I or T has been reported by several investigators to be a strong indicator for the absence of cardiac injury in patients with blunt chest trauma.3,5,7,8
To diagnose a cardiac contusion, the ideal timing of blood sampling for troponin assays has not yet been determined. Some investigators found that both troponin I and troponin T can reach peak values earlier following cardiac trauma than after acute myocardial infarction.3,26 However, if troponin I or T concentrations are within reference ranges on admission shortly after trauma, a secondary measurement after 4–6 hours is necessary to reliably exclude myocardial injury.26 Increased troponin I or T may persist for 4–6 days and thus may also facilitate an evaluation for cardiac damage of patients presenting days after the injury.3
ELECTROCARDIOGRAPHY
The ECG after blunt chest trauma may be normal or may show non-specific abnormalities (table 1).2–5,12–15,17 Because of its anterior position in the thorax and proximity to the sternum, the right ventricle is far more frequently injured than the left ventricle.1,6,7,9,17,20,27 The ECG mainly reflects the electrical activity of the left ventricle because of its greater mass. The ECG is relatively insensitive to right ventricular electrical activity. For that reason, a cardiac contusion usually results in moderate right ventricular damage with only minor electrical changes, which can easily be missed on an ECG. Disappointingly, in a study by Walsh and colleagues,28 patients with and without blunt chest trauma could not be differentiated by right precordial lead recording (V4R).28
Electrocardiographic findings in cardiac contusion
Non-specific ECG abnormalities are often seen in trauma patients. Some of these ECG changes may be caused by non-cardiac factors such as hypoxia, anaemia, abnormal concentrations of serum electrolytes, and changes in vagal or sympathetic tone.
Left ventricular injury can produce ST segment or T wave abnormalities or, in the case of extensive necrosis, new Q waves.4,13 Some ECG changes that require treatment appear only after several hours. So, at least one repeat ECG is recommended.13,14
A severely injured right ventricle may cause a right bundle branch block, usually transient.1,13,17 Less commonly, various degrees of atrioventricular block have been documented after blunt chest trauma.1,4,13,17 In addition, myocardial cell damage produces electrical instability, which may result in a variety of supraventricular or ventricular arrhythmias.4,6,13 Sinus tachycardia and ventricular and atrial extrasystoles are the most frequently reported rhythm disorders. More serious arrhythmias such as atrial fibrillation, ventricular tachycardia, and ventricular fibrillation occur less often but may acutely compromise the haemodynamic state or even result in sudden death.4
ECHOCARDIOGRAPHY
Contused myocardial tissue not only resembles infarcted myocardial tissue histologically but also functionally.13 A myocardial contusion can be recognised by localised myocardial wall dysfunction. Consequently, two dimensional echocardiography, which provides a direct view of wall motion abnormalities, has been shown in several studies to be an excellent tool in the detection of cardiac injury (table 2).1,2,9,27 In addition, echocardiography may show associated valvar lesions, intracardiac shunts or thrombosis, pericardial effusion or tamponade, and ventricular dilatation.1,2,6,12,27,29 From a practical standpoint, other important advantages of echocardiography are its non-invasive nature and its ease of use at the bedside and in the emergency department. However, in patients with painful chest wall injuries transthoracic echocardiographic access may be limited. In these patients transoesophageal echocardiography (TOE) can be performed.9,11,12,29 Although TOE is risky because of the insertion of the probe in to the oesophagus and the frequent need for sedation of the conscious patient, it has been shown to be safe in the evaluation of patients who have suffered blunt chest trauma. Two studies reported no complications respectively in 68 and 117 TOE procedures performed on severely injured trauma patients.11,12 Another study in critically ill intensive care patients described worsening of haemodynamics and respiratory difficulties with TOE in two patients (4%) who had heart failure.30 TOE is also recommended in case of suspected lesions to the great vessels or if the transthoracic images are suboptimal. Standard two dimensional echocardiography cannot detect minor injury with only myocardial oedema but no wall motion abnormalities. This entity, often referred to as cardiac “concussion”, however, can possibly induce life threatening arrhythmias.4,6
Echocardiographic findings in acute cardiac contusion
RADIONUCLIDE IMAGING
Ventriculography
Because of the increased availability of echocardiography, the use of radionuclide ventriculography to detect wall motion abnormalities and determine ejection fractions has been largely abandoned.15,17,31,32
Myocardial perfusion scintigraphy
In the past, the ability of myocardial perfusion scintigraphy to detect perfusion defects was investigated for its value in the diagnosis of a cardiac contusion.33–38 The initial planar 99m-Tc pyrophosphate imaging studies were reported to have low sensitivity for cardiac injury because these scans showed only large transmural defects.37,38 Later studies using 201-thallium single photon emission computed tomography (SPECT) were more precise in the detection and localisation of small transmural and non-transmural defects of the left ventricular wall.33–36 However, because the right ventricle is poorly visualised with 201-thallium SPECT, an isolated right ventricular contusion can theoretically be missed. The value of myocardial perfusion scintigraphy in the setting of an acute cardiac contusion therefore remains limited.
Positron emission tomography
Positron emission tomography has been shown to have great advantages in the assessment of myocardial viability in general. However, no experience with positron emission tomography in patients with blunt chest trauma has been reported in the literature.39
IDENTIFICATION OF PATIENTS AT RISK
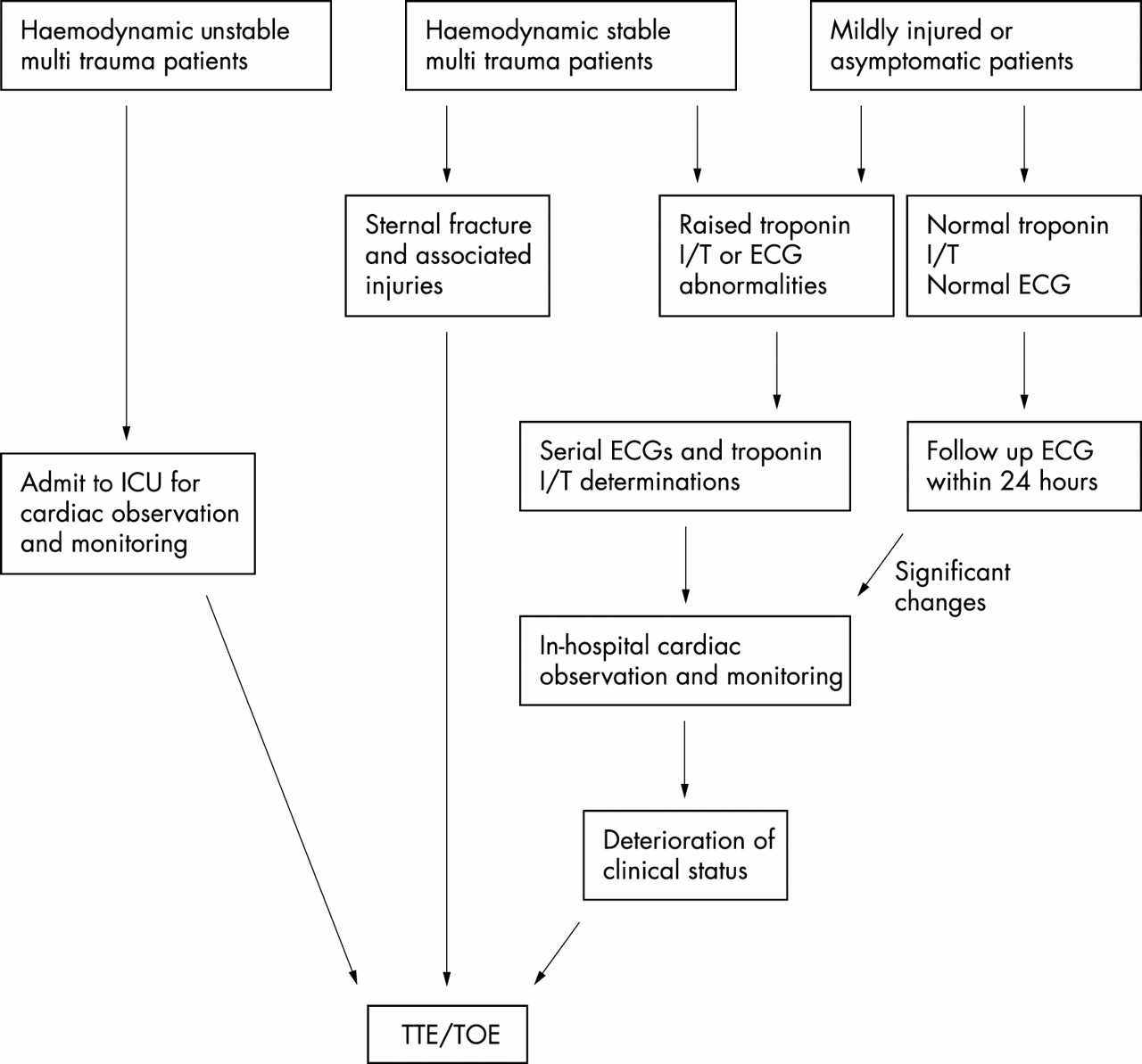
None of the older diagnostic tests mentioned above were found to be accurate enough to confirm a cardiac contusion or to be precise enough to predict all complications (table 3). However, the latest studies show that troponin I and troponin T are very helpful in the stratification of patients at risk for such complications.3,5,8 On the basis of these new data we suggest the following screening strategy, which is also illustrated in fig 1.
Early and late complications of cardiac contusion
{kind=link}
Screening strategy to identify patients at risk for cardiac complications in relation to the severity of associated injuries. ICU, intensive care unit; TOE, transoesophageal echocardiography; TTE, transthoracic echocardiography.
Firstly, severely injured patients who present with haemodynamic instability must be suspected of having structural damage to the heart, the great vessels, or both and should have an echocardiographic examination as soon as possible.3,6,9,11,12
Secondly, for haemodynamically stable patients with multiple trauma, it is important to note that an isolated sternal fracture is not necessarily a sign of cardiac injury.2,40 However, in severely injured patients a sternal fracture may indicate cardiac injury and echocardiographic evaluation is recommended in these patients.41,42 A small pericardial effusion associated with a sternal fracture, which is probably caused by pericardial irritation, neither implies cardiac injury nor increases the risk of tamponade.41,42 Increased concentrations of cardiac troponin I and troponin T or ECG abnormalities indicate a higher risk of developing cardiac complications. Further investigation including echocardiography, serial ECGs, and troponin I determinations is advised.3,4,8,12
In a third group, consisting of mildly injured and asymptomatic patients, increased concentrations of CK-MB, troponin I or T, and minor ECG abnormalities do not necessarily indicate a clinically significant cardiac contusion because not all these patients will develop complications.3,5,8,14,24,25 On the other hand, a normal concentration of cardiac troponin I or T rules out cardiac damage and consequently minimises the risk of cardiac complications.3,5,8 Therefore, in-hospital monitoring may be limited to patients with increased troponin concentrations or with significant ECG abnormalities. Serial ECGs and troponin determinations are advised until the results turn normal.3,5 Echocardiography has rarely shown clinically significant functional or structural cardiac injuries in this group of patients.1,2,4,14,27 Echocardiography is very useful if the patient’s clinical status deteriorates or if there is a discrepancy between clinical status, ECG, and cardiac enzyme concentrations.1,4
TREATMENT OF CARDIAC INJURY
If in-hospital cardiac monitoring is necessary, the hospitalisation period can be limited because nearly all (81–95%) life threatening ventricular arrhythmias and acute cardiac failures occur within 24–48 hours after the trauma.5,9,14
Treatment of a cardiac contusion in severely injured patients consists of haemodynamic stabilisation and treatment of associated injuries. In case early surgery is required general anaesthesia can be safely used. Within the first month following injury strict intraoperative haemodynamic monitoring is advisable.1,2,4,6,14,43
PROGNOSIS
Prognosis of patients in whom a cardiac contusion is diagnosed following a blunt chest trauma has been reported to be favourable. Severe cardiac injury with myocardial necrosis heals by scar formation, similar to that in ischaemic myocardial infarction. This may lead to ventricular aneurysm formation and in some cases to chronic heart failure.6,44,45 A previous cardiac contusion must be taken into consideration in case of unexplained dilated cardiac dysfunction (especially if the right ventricle is affected), aneurysms of the ventricles or coronary arteries, unexplained constrictive pericarditis, or valvar lesions.16,22,44–46
CONCLUSION
Diagnosing a cardiac contusion remains a significant challenge. Previously, none of the available diagnostic tests were sensitive or specific enough to determine cardiac injury. Nowadays, however, with the widespread availability of the cardiospecific troponin I and troponin T assays it has become much easier to detect myocardial injury, especially in the category of patients without evident signs of cardiac injury. Troponin I and troponin T have also facilitated the stratification of patients at risk for life threatening complications. A troponin I or T assay in combination with an ECG was shown to be sufficient for identifying the vast majority of patients who were at risk, thus avoiding extensive diagnostic screening. Moreover, patients with normal troponin I or T concentrations and ECG can be safely sent home. On the basis of these new data, we have proposed a screening protocol with different diagnostic strategies according to the severity of associated non-cardiac injuries.
REFERENCES
Linked Articles
- Miscellanea