Article Text

Abstract
Objective: To determine the epidemiology of out of hospital sudden cardiac death (OHSCD) in Belfast from 1 August 2003 to 31 July 2004.
Design: Prospective examination of out of hospital cardiac arrests by using the Utstein style and necropsy reports. World Health Organization criteria were applied to determine the number of sudden cardiac deaths.
Results: Of 300 OHSCDs, 197 (66%) in men, mean age (SD) 68 (14) years, 234 (78%) occurred at home. The emergency medical services (EMS) attended 279 (93%). Rhythm on EMS arrival was ventricular fibrillation (VF) in 75 (27%). The call to response interval (CRI) was mean (SD) 8 (3) minutes. Among patients attended by the EMS, 9.7% were resuscitated and 7.2% survived to leave hospital alive. The CRI for survivors was mean (SD) 5 (2) minutes and for non-survivors, 8 (3) minutes (p < 0.001). Ninety one (30%) OHSCDs were witnessed; of these 91 patients 48 (53%) had VF on EMS arrival. The survival rate for witnessed VF arrests was 20 of 48 (41.7%): all 20 survivors had VF as the presenting rhythm and CRI ⩽ 7 minutes. The European age standardised incidence for OHSCD was 122/100 000 (95% confidence interval 111 to 133) for men and 41/100 000 (95% confidence interval 36 to 46) for women.
Conclusion: Despite a 37% reduction in heart attack mortality in Ireland over the past 20 years, the incidence of OHSCD in Belfast has not fallen. In this study, 78% of OHSCDs occurred at home.
- AED, automated external defibrillator
- CAD, coronary artery disease
- CI, confidence interval
- CPR, cardiopulmonary resuscitation
- CRI, call to response interval
- EMS, emergency medical services
- OHCA, out of hospital cardiac arrest
- OHSCD, out of hospital sudden cardiac death
- PAD, public access defibrillation
- SCD, sudden cardiac death
- VF, ventricular fibrillation
- sudden cardiac death
- ventricular fibrillation
Statistics from Altmetric.com
- AED, automated external defibrillator
- CAD, coronary artery disease
- CI, confidence interval
- CPR, cardiopulmonary resuscitation
- CRI, call to response interval
- EMS, emergency medical services
- OHCA, out of hospital cardiac arrest
- OHSCD, out of hospital sudden cardiac death
- PAD, public access defibrillation
- SCD, sudden cardiac death
- VF, ventricular fibrillation
Despite improvements in diagnosis and management over the past three decades, coronary artery disease (CAD) is the major cause of death in the western world.1 The majority of CAD deaths occur outside of hospital,2 with the largest component being sudden cardiac death (SCD).3
The current definition of SCD describes death within one hour of onset of symptoms.4 From a practical viewpoint estimating the duration of the symptoms that preceded death is often very difficult among patients found “dead on arrival”. Often information is lacking about the occurrence and timing of any symptoms, and for many out of hospital SCDs (OHSCDs) the emergency medical services (EMS) are not deployed. For these reasons the true incidence of OHSCD is difficult to ascertain.
Forensic pathologists studying unwitnessed deaths may use the definition “sudden” for the death of a person known to have been alive and functioning normally 24 hours before.5 The exclusion of unwitnessed deaths seriously biases any study of OHSCD.6 World Health Organization criteria define SCD as unexpected death either within one hour of symptom onset if witnessed or within 24 hours of the person having been observed alive and symptom-free if unwitnessed.7 For these reasons many studies of the incidence of SCD and out of hospital cardiac arrest (OHCA) based only on witnessed cases (or the one hour definition) may be underestimating the full extent of the problem.
Investigators have shown that prospective evaluation of SCD based on necropsy reports, EMS patient report forms, and medical records appears to give a more accurate determination of incidence than retrospective evaluation of death certification data, which can overestimate SCD incidence.7
World Health Organization statistics show that deaths from heart attacks in Ireland have fallen by 37% in the past 20 years.8 Finnish investigators have claimed that a decline in out of hospital CAD deaths has been the leading contributor to the decrease in CAD deaths.2 By using EMS patient report forms, Becker et al9 noted that the incidence of OHCA attended by EMS varied between 36 and 128/100 000 a year. Investigators in Maastricht found the mean yearly incidence of OHCA to be 97/100 000.10 The task force on SCD of the European Society of Cardiology stated that the incidence of SCD ranged between 36–128/100 000 inhabitants a year.11 Investigators assessed deaths from CAD in Belfast and nearby Castlereagh local government districts in 1982 by checking EMS patient report forms, death certification data, and necropsy reports.12 Of 335 OHSCDs, 82% occurred in the home and 67% were due to a “presumed ventricular arrhythmia”. In 1966, earlier investigators had shown that there were 297 CAD deaths within one hour of symptom onset in Belfast City.13
The initial rhythm for most OHCAs (65–85%) is ventricular fibrillation (VF).14 The greatest determinant of survival from OHCA is early defibrillation.15 Work in the UK has shown that fewer than 5% of victims of OHCA have been resuscitated with the commonly used EMS approach.16 However, this figure arises from an assessment of all OHCAs. In Gothenburg, a 19 year study showed a 13% survival rate for patients having a witnessed OHCA and 20% for witnessed OHCA with VF as the initial rhythm.17
The Utstein guidelines recommend reporting the survival rate from witnessed OHCA of cardiac aetiology with VF as the initial rhythm for intersystem comparisons.17,18 Survival from OHCA has been shown to be improved significantly by means of a public access defibrillation (PAD) scheme with automated external defibrillators (AEDs).19
The joint European Society of Cardiology/European Resuscitation Council guidelines on the use of AEDs in the community state that local conditions should be analysed before setting up a PAD scheme to help decide on the best strategy for AED deployment in the community.20
The purpose of this study was to determine the incidence and demographics of OHSCD occurring in Belfast City and Castlereagh local government districts over one year (August 2003 to July 2004) to determine the current survival rate from OHSCD and to use the demographics of OHSCD to help determine the best strategy for AED deployment for the implementation of a PAD scheme. In Belfast OHSCD had not been looked at since 1966 and 1982.
METHODS
Between August 2003 and July 2004 data were collected prospectively for OHCAs of a suspected cardiac aetiology in Belfast City and neighbouring Castlereagh local government districts in which the EMS system responded and attempted resuscitation. All patient report forms in these areas were searched manually. OHCAs were reported in the Utstein style.18 In addition, investigators prospectively searched through all necropsy reports at the department of forensic medicine at the Royal Victoria Hospital, Belfast. No age groups were excluded from the investigation.
Data collected from EMS patient report forms were patient demographics, medical history, the timing of symptoms, and when the patient was last seen alive. Details gathered on the arrests were whether it was witnessed, bystander cardiopulmonary resuscitation (CPR), rhythm on EMS arrival, attempted defibrillation, resuscitation status (defined as admission to hospital alive), and survival status (discharged from hospital alive). Investigators also recorded the time of emergency telephone call and the time that the EMS vehicle reached the site of the OHCA, with the time difference defined as the call to response interval (CRI) (a surrogate measurement of collapse to shock time).18 At the time of the study, most of the EMS vehicles in Belfast did not have data reading facilities for defibrillators and the time of collapse is available only for witnessed arrests (which can be unreliable). CRI was rounded to the nearest minute.
For each OHCA, investigators also recorded the site of the event as home (any private place of residence), nursing homes, indoor public place, outdoor public place, and public or private transport.
For patients admitted to hospital, medical records were checked and if the patients were discharged alive, the neurological status on discharge was noted. Neurological status coding was based on work by previous investigators and had four functional levels: level 1 (full or nearly full neurological recovery, including patients with minor short term memory loss); level 2 (major memory deficit, naming difficulty, coordination difficulty, requiring some help with activities of daily living); level 3 (patient alert and awake but with major neurological impairment and fully dependent for activities of daily living); and level 4 (unresponsive and comatose).19,21
For patients whose medical history was not available from the patient report form the patient’s general practitioner was contacted.
To help ascertain that each OHCA was of a cardiac aetiology and satisfied criteria for SCD, all obviously non-cardiac cases were excluded, including overdoses, suicides, smoke inhalation, trauma, obvious severe asthma attacks, and terminal cancer. Cardiac aetiology of OHCAs was clarified from necropsy reports and death certification data. Three cardiologists assessed cases independently to reach a consensus opinion on whether each case (300) met the criteria for SCD.
Cases were deemed to be “sudden” and therefore OHSCDs if they satisfied World Health Organization criteria.7 We also considered deaths to be sudden if the person had been seen alive and asymptomatic within 24 hours of being found collapsed but the EMS was not called and postmortem examination found cardiac abnormality. Death certificates with cardiac causes for patients found dead for whom the EMS was not called and who had no necropsy were not included in the analysis, as previous work has shown that reliance on death certificate diagnoses alone overestimates the true rate of SCD.
The study area
Belfast is a medium sized city. According to mid year population estimates in 2003 the population of Belfast City local government district was 271 596. Castlereagh is a neighbouring suburban area to the east of the city with a population of 66 076; therefore, the combined population of the study area is 337 672.22 According to the 1971 census the population of Belfast City was 416 679.22 As the boundaries of Belfast City local government district have changed and now cover a smaller area, the decline in population from 1971 is apparent. In 1971 Belfast City included parts of what is now Castlereagh.
The emergency medical services
Belfast and Castlereagh local government districts had no PAD scheme in place at the time of the study and the police and fire brigade were not a part of the EMS system. Belfast and its surrounding suburbs are served by two mobile coronary care units (doctor led): one based at the Royal Victoria Hospital, which covers the north, west, and south of the city; and the other at the Ulster Hospital, which covers the east of the city and Castlereagh. The mobile coronary care units provide rapid out of hospital assessment of acute ischaemic-type chest pain and of collapsed patients and provide thrombolytic treatment and defibrillation. Belfast City is also served by four ambulance stations, which house emergency paramedic led ambulances. The paramedic led ambulances provide a rapid defibrillation service. For most OHCAs the emergency dispatcher sends an emergency paramedic led ambulance in conjunction with the mobile coronary care unit, aiming at reaching all patients within eight minutes of the call. In most cases the paramedic led ambulances administer initial defibrillatory shocks and CPR. The EMS in Belfast City use biphasic defibrillators with 150 J of non-escalating energy protocols.
There are a few fixed AEDs in Belfast City. Most of these static AEDs are located in places such as golf clubs and private leisure centres. During this study none of these static AEDs were used for collapse victims. Some general practitioner practices have AEDs and use of one of these resulted in survival from OHSCD during the study.
Statistical analysis
European age standardised incidence and world age standardised incidence were calculated for men and women. The 95% confidence interval (CI) associated with each rate is also presented. Population denominators used in the calculation of these rates were obtained from the Northern Ireland Statistics and Research Agency website.22
Significance for means was calculated by the t test in the statistical package SPSS version 12 (SPSS Inc, Chicago, Illinois, USA).
RESULTS
There were 300 OHSCDs over the 12 months (197 (66%) in men). Overall mean (SD) age was 68 (14) years (range 27–96 years), with a mean age for women of 72 (13) years and for men of 65 (14) years (table 1).
Distribution of all cases of out of hospital sudden cardiac death by age and sex of patient
One hundred and thirty (43%) had a medical history of cardiac disease; for eight of the 300 (2.7%) OHSCD a history of the patient was unobtainable. Two hundred and thirty four (78%) OHSCDs occurred at home, 24 (8%) in outdoor public places, 23 (7.7%) in indoor public places, and 19 (6.3%) in nursing homes. Two hundred and seventy nine (93%) of the victims of OHSCDs were attended by the EMS. Of the 279 EMS attended patients, initial rhythm on EMS arrival was asystole in 190 (68%), VF in 75 (27%), and pulseless electrical activity in 14 (5%) (table 2).
Rhythm on arrival of emergency medical services
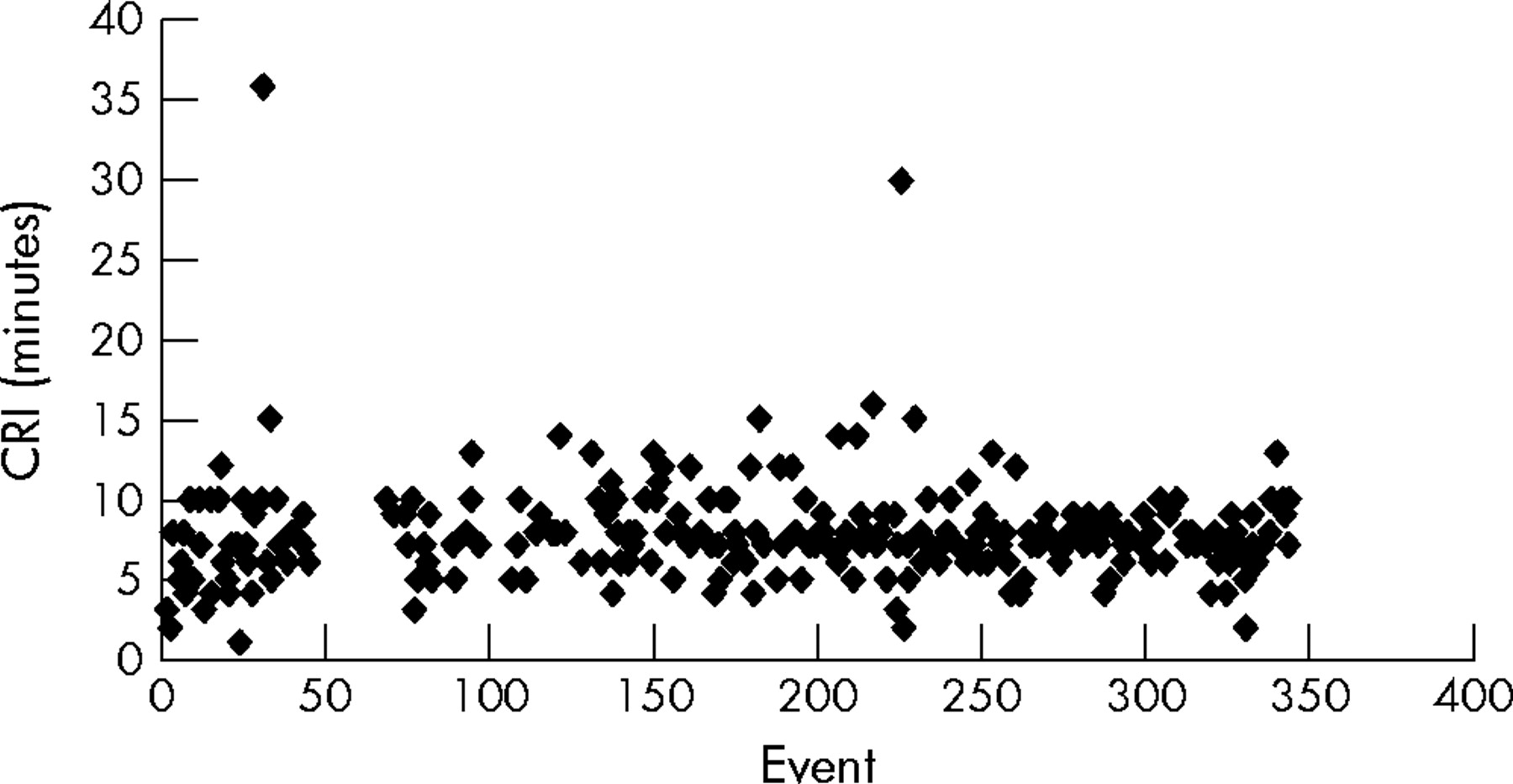
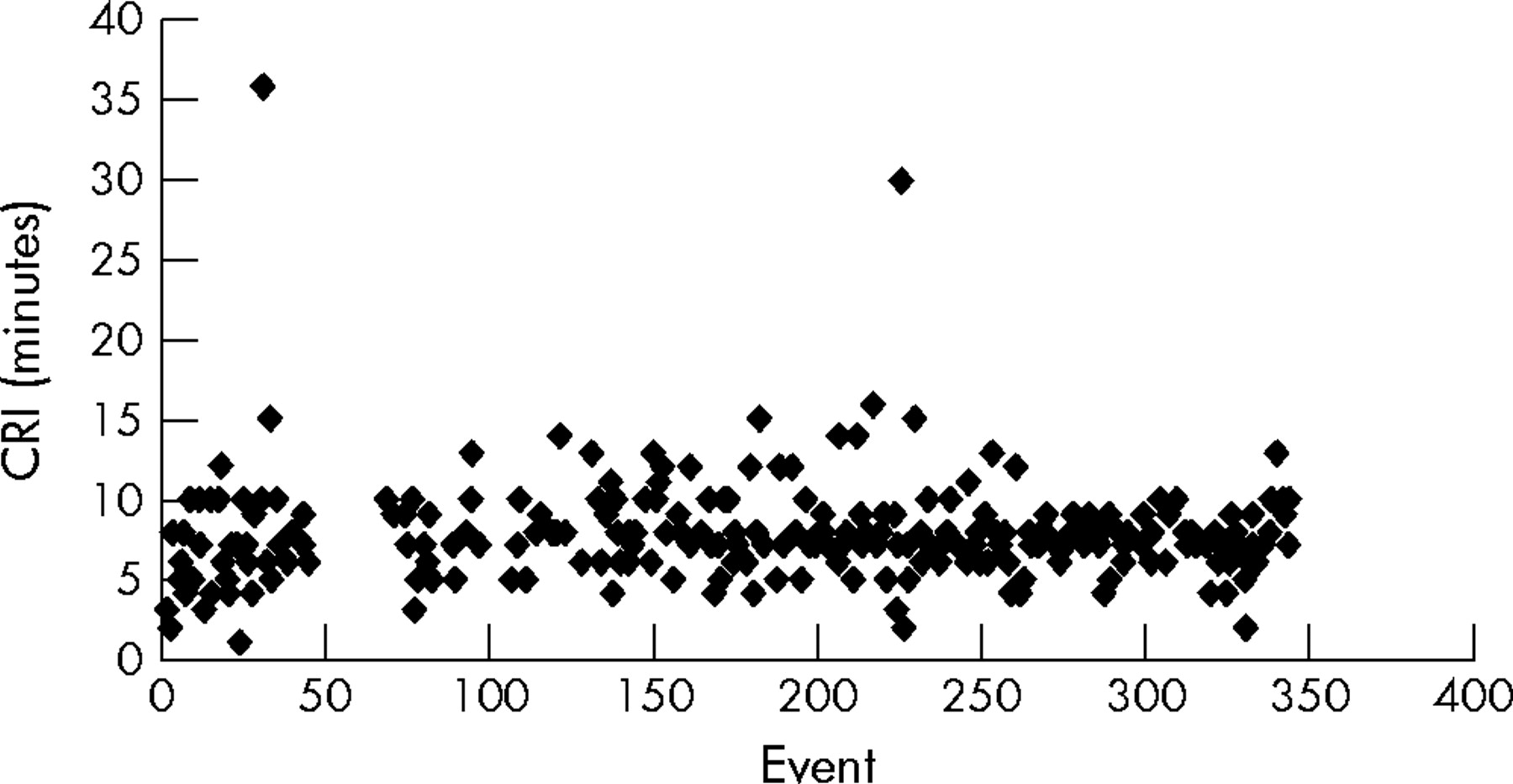
The CRIs ranged from 1–36 minutes (mean (SD) 8 (3) minutes). Median CRI was 7 (interquartile range (IQR) 6–9) minutes. For 200 (71.7%) of the 279 patients CRI was ⩽ 8 minutes (fig 1). For patients attended by the EMS, the resuscitation rate was 27 of 279 (9.7%) and survival rate 20 of 279 (7.2%). The CRI for survivors was mean (SD) 5 (2) minutes and for non-survivors mean (SD) 8 (3) minutes (p < 0.001). Median CRI for survivors was 5 (IQR 4–6) minutes and for non-survivors 7.5 (IQR 7–9) minutes.
{kind=link}
Scatter graph showing the distribution of call to response intervals (CRI) for the emergency medical services.
Ninety one (30%) OHSCDs were witnessed. Forty eight (53%) of the patients with witnessed arrests had VF on EMS arrival (table 2). Only 92 of 279 (33%) patients having arrests received bystander CPR, and for 12 of 279 (4.3%) bystander CPR status was not known. The survival rate for patients with arrests receiving bystander CPR was 13 of 92 (14.1%). Survival rate for witnessed VF arrests was 20 of 48 (41.7%). All 20 survivors had witnessed arrests, VF as the initial rhythm, and a CRI ⩽ 7 minutes.
The European age standardised incidence for OHSCD for men was 122/100 000 (95% CI 111 to 133). The analogous rate for women was 41/100 000 (95% CI 36 to 46). The world age standardised incidence for OHSCD was 89/100 000 (95% CI 81 to 97) for men and 29/100 000 (95% CI 25 to 32) for women.
Of the 20 survivors, 13 (65%) had full neurological recovery with a neuroscore of 1, one patient had a neuroscore of 2, two had a neuroscore of 3, and four (20%) were comatose with a neuroscore of 4.
For the 300 OHSCDs, 110 necropsy reports were available (table 3).
Necropsy findings for out of hospital sudden cardiac deaths (n = 110)
Necropsy reports were as follows: 103 (93.6%) coronary artery atheroma with ⩾ 70% stenosis in at least one of the three main coronary arteries, 28 (25.4%) coronary artery thrombus and plaque rupture, 28 (25.4%) healed or fibrotic myocardial infarcts, 26 (23.6%) acute myocardial infarcts, 53 (48%) cases of left ventricular hypertrophy, and four cases of ruptured myocardial infarct with haemopericardium; in one 27 year old man, the heart was grossly and histologically normal.23 Of the seven patients without a coronary stenosis of ⩾ 70% in at least one vessel, one had moderate coronary artery atheromatous disease with 30% stenoses and six had no significant coronary artery atheroma.
Of the 20 patients who survived to discharge, eight had ST segment elevation myocardial infarction, four had non-ST segment elevation myocardial infarction, three had idiopathic dilated cardiomyopathy, two had ischaemic cardiomyopathy, one had severe mitral valve disease, and one had atrial leiomyosarcoma; for one patient the diagnosis was uncertain.
DISCUSSION
The premise of the National Service Framework for CAD in the UK was to reduce the death rate from circulatory diseases such as myocardial infarction in people under 75 years by 40% by 2010. The death rate has already been reduced by 23.4% from the 1995–7 baseline.24 Since 1970 CAD deaths have fallen in general across Western Europe.25 Nevertheless, the percentage of CAD deaths that are sudden has increased from 38% to 47%.26 Despite recent advances in technology survival from OHSCD remains low throughout the world at about 5%.19,26
OHSCD is often unexpected and may be the first and only manifestation of CAD, occurring in apparently healthy, asymptomatic people, and therein lies the problem for its prevention. In this study 162 of the 300 victims of OHSCD (54%) had no known history of cardiac disease. However, almost 94% of the necropsy reports showed severe CAD with at least 70% stenosis in one or more of the three main coronary arteries. The greatest opportunity, therefore, to reduce the population burden of OHSCD lies in further reduction in the prevalence of CAD in the population by prevention and risk factor modification. The risk factors for SCD have been shown to be largely the same as those for CAD.11 The role of hypertension with regard to SCD is disproportionate to that of CAD.27 The hazard ratio of hypertension for SCD was 1.45 (95% CI 1.10 to 1.92, p = 0.008) for each 50 g/m increment in left ventricular mass in the Framingham study.28 In our study 48% of necropsies of OHSCD victims showed left ventricular hypertrophy.
Previous investigators have looked at supplying AEDs to the homes of people with known CAD and at risk of ventricular arrhythmias and training family members in their use. Some early experience with home AEDs showed no benefit.29 Most victims of SCD have no known CAD and patients with known CAD who are at risk of SCD may be eligible for implantable cardioverter-defibrillators,30 thereby limiting the potential for home AEDs.
The greatest impediment to survival from OHSCD is prolonged CRIs for the EMS. One of the solutions suggested is to increase EMS capabilities and vehicles. But to improve EMS response times would be costly and it has been estimated that every second of improved EMS response would cost about £28 000.31 A more cost effective means of improving time to defibrillation may be PAD, since most OHSCDs occur in the home. Such programs would require mobile AEDs and first responders linked to a dual dispatch system with the local EMS.19
This study and others have shown a decline in the proportion of OHSCDs with VF as the initial rhythm.32 However, the percentage of witnessed OHSCDs with VF as the initial rhythm was much higher (53%), suggesting that the initial mechanism for most OHSCDs is still arrhythmic in nature. High levels of asystole are due to prolonged CRIs and the high proportion of unwitnessed arrests (which may have been pulseless for an undetermined period of time).
The limitations of this study are common to many, mainly arising from incomplete data. We have tried to minimise this. The study did not consider any death certificates of people found dead for whom the EMS was not called, meaning that a small number of OHSCDs may have been missed. However, to have included all these cases would have resulted in overestimation of the incidence of OHSCD.
The European age standardised incidence for OHSCD in our study was 122/100 000 for men and 41/100 000 for women. The age standardised incidence of OHSCD in Belfast in 1966 is not available. However, the rate of OHSCDs was 71/100 000 population in Belfast in 1966. Because no age standardised incidence is available for OHSCD in 1966 our data cannot be directly compared. However, even allowing for an aging population, the incidence of OHSCD in Belfast City over the past 38 years does not appear to have fallen.
Acknowledgments
This study was supported by a Royal Victoria Hospital fellowship and by the Investing for Health grant from the Research and Development office of Northern Ireland. The authors thank the Northern Ireland Statistics and Research Agency, The Department of Forensic Medicine at the Royal Victoria Hospital, Belfast, and the Northern Ireland Ambulance Service for their help in obtaining data.
REFERENCES
Footnotes
-
Published Online First 6 June 2005
-
None of the authors have any competing interests to declare
-
The study complied with the Declaration of Helsinki and received approval from the local research ethics committee, Royal Victoria Hospital, Belfast