Article Text

Abstract
Aims: To determine the relevance of lymphopenia to the diagnosis of bacteraemia in patients admitted with medical emergencies, relative to peripheral blood white cell count and neutrophilia.
Patients/Methods: A two year cohort study carried out in a teaching hospital in Oxford, UK of 21 495 consecutive adult emergency admissions to general medical or infectious disease wards. Full blood data were available in 21 372 cases; 41 cases with extreme full blood count results (neutrophil count, > 75 × 109/litre; lymphocyte count, > 10 × 109/litre) were excluded, leaving 21 331 cases for analysis. The association between the admission lymphocyte and neutrophil counts and the risk of bacteraemia was assessed.
Results: Neutrophilia and lymphopenia were both associated with bacteraemia. Lymphopenia was the better predictor in this cohort. Both neutrophilia and lymphopenia were more predictive of bacteraemia than the total white blood cell count.
Conclusions: Both lymphocyte and neutrophil counts, rather than total white blood cell count, should be considered in adult medical admissions with suspected bacteraemia.
- AUC, area under the curve
- HIV, human immunodeficiency virus
- ROC, receiver operating characteristic
- WBC, white blood cell count
- lymphopenia
- blood cell count
- sensitivity and specificity
- bacteraemia
Statistics from Altmetric.com
- AUC, area under the curve
- HIV, human immunodeficiency virus
- ROC, receiver operating characteristic
- WBC, white blood cell count
Alterations of white blood cell count (WBC) are well recognised features of sepsis,1 and raised WBC and neutrophilia are associated with bacteraemia in both adults2 and children.3,4 A rapid, profound lymphopenia occurs in primates with experimental bacteraemia.5–7 Recent clinical studies, performed on groups at low human immunodeficiency virus (HIV) risk, suggest that lymphopenia may define patients at high risk of adverse outcome. For example, lymphopenia is a risk factor for intensive care in unwell infants,8 and for death in nursing home residents with pneumonia.9
“The existing literature on the relation between lymphopenia and bacteraemia is difficult to evaluate”
In view of this, we investigated whether lymphopenia was useful for predicting bacteraemia clinically, an activity that remains imprecise even after detailed study.2,10 The existing literature on the relation between lymphopenia and bacteraemia is difficult to evaluate: two observational studies, involving a total of about 750 elderly patients, have noted lymphopenia in some patients with bacteraemia, but specificity varied between the studies, and the distributions of the counts were not reported.11,12 Generalisation of the published data to other populations is further complicated by the gradual decline in lymphocyte counts that occurs as normal adults age.13,14 We sought to clarify the relation between age, lymphocyte count, neutrophil count, and bacteraemia by the study of a large cohort of adults with medical emergencies in a region, which, at the time of study, had a low prevalence of HIV.
METHODS
Study design and setting
The cohort studied comprised consecutive patients, aged at least 18 years, admitted from the community as emergencies to general medical or infectious diseases services of the Oxford Radcliffe Hospital, UK, from 1 February 1999 to 31 January 2001. Patients admitted to haematology or cardiology wards did not form part of the cohort because admission to these wards usually implies either known haematological disease or an acute coronary syndrome.
Microbiology and haematology
Blood cultures were taken by medical staff if thought to be clinically indicated, using pairs of anaerobic and aerobic Bactec F+ bottles (Becton-Dickinson, Oxford, UK). Bottles were incubated for five days, unless endocarditis was suspected, when 21 day incubations were used. Isolates were speciated by routine methods. Admission cultures were defined as those taken in the first two days of admission. Full blood counts were performed using a Technicon H3 analyser (Bayer, Newbury, UK). The clinical laboratories involved in specimen processing were accredited by the UK Clinical Pathology Accreditation scheme.
For the purposes of our study, we considered “significant isolates” as any blood culture yielding an organism other than a coagulase negative staphylococcus or Corynebacterium spp. These isolates are unlikely to reflect genuine bacteraemia in the population studied, in which line related sepsis is very rare. Mixed cultures were considered significant if organisms other than coagulase negative staphylococcus or Corynebacterium spp were isolated.
Data collection and analysis
Data used in the study were recorded during the patients’ admissions on the hospital’s information systems, and abstracted in an anonymous form. Analysis was performed at the end of the study period.
Statistical methods
SPSS version 11 was used for logistic regression and receiver operating characteristic (ROC) plotting. ROC plots displayed sensitivity versus 1-specificity, such that the areas under the curve (AUCs) generated varied from 0.5 to 1.0, with higher values indicating increased discriminatory ability. Confidence intervals on AUCs of ROC plots were calculated using non-parametric assumptions. The odds of significant bacteraemia for a given group of patients were calculated as: cases of significant bacteraemia/cases without significant bacteraemia. For univariate and multivariate logistic regression analysis, a variable was calculated to represent the distance between the observed lymphocyte and neutrophil counts and a count in the normal range (7 × 109/litre and 2 × 109/litre, respectively). This variable, calculated as ((neutrophils) − 7 × 109/litre) × (2 × 109/litre − (lymphocytes))/1 × 109/litre), increases as lymphocytes fall and neutrophils rise.
RESULTS
Composition of the cohort
There were 21 495 patients and 21 331 were analysed further. Figure 1 shows the reasons for exclusion. Ages ranged from 18 years to 106 years; the average inpatient stay was 6.4 days. Admission cultures were obtained from 7182 (33.6%) patients. Of these, in 5964 cases (83.0%), a single pair (aerobic and anaerobic) was used. Significant isolates were isolated from 530 patients. There were 520 cases of coagulase negative staphylococcus and 39 cases of Corynebacterium spp; these were considered contaminants. Table 1 shows the numbers of patients, their ages, and the blood culture isolates obtained.
Blood culture isolates obtained
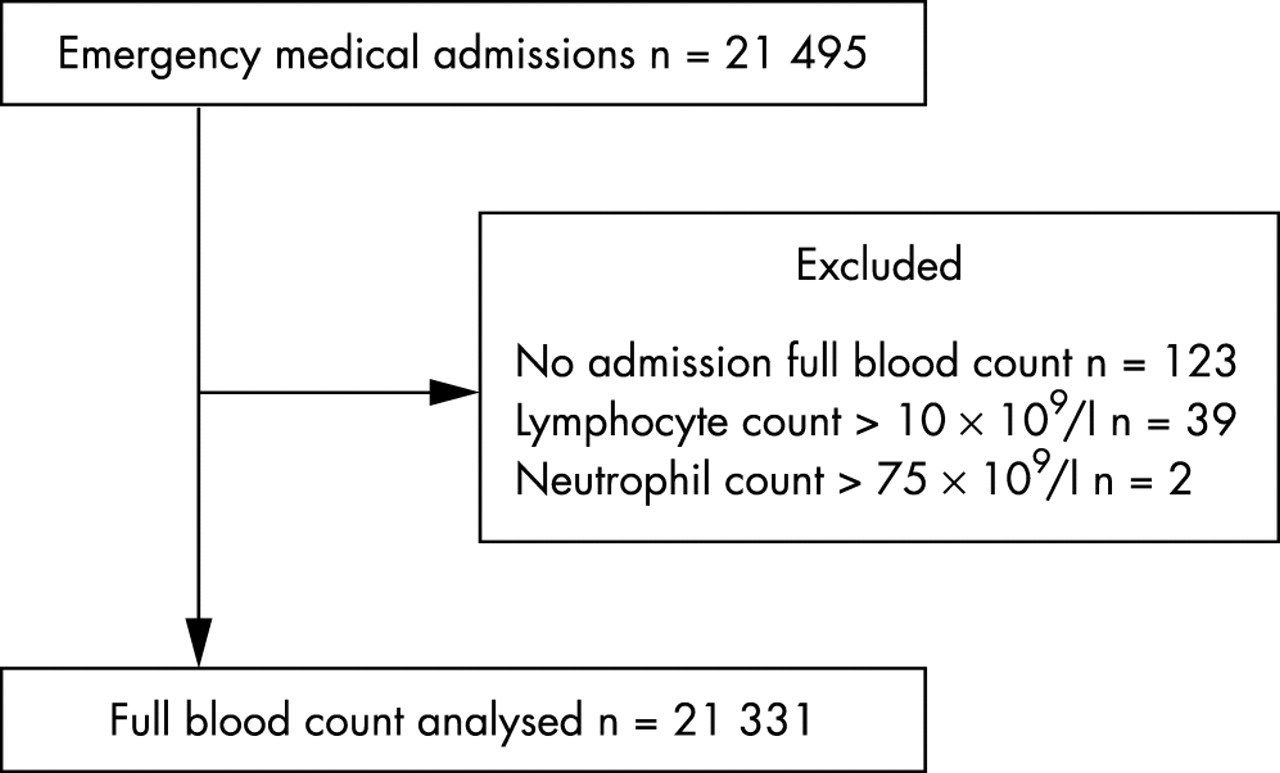
Cases analysed. The reasons for exclusion of cases, and the distribution of lymphocyte and neutrophil counts within the cohort are shown.
Association between age, bacteraemia, and cell counts
In our cohort, the peripheral lymphocyte count declined with age (fig 2), as described previously.13,14 However, at all ages, the lymphocyte count was highest in those in whom cultures were not performed, intermediate in those in whom cultures were taken but no significant isolate obtained, and lowest in the patients with bacteraemia (fig 2A).

Neutrophil and lymphocyte counts by age. Age stratified lymphocyte and neutrophil counts among non-cultured, culture negative, and culture positive patients are shown. Symbols indicate the admission value; errors are standard errors of the mean. Table 1 shows the numbers of cases at each point.
Change in lymphocyte count during admission
We considered whether the lymphopenia that we observed was, as predicted by experimental data,5,6 a transient phenomenon, or whether it represented a pre-existing condition predisposing to bacteraemia. Admission blood counts were compared with the last count taken during the admission. Figure 2 shows that, during admission, both the admission neutrophilia and lymphopenia seen in the patients with bacteraemia declined, compatible with both changes being a response to bacteraemia.
Lymphocyte and neutrophil counts and bacteraemia risk
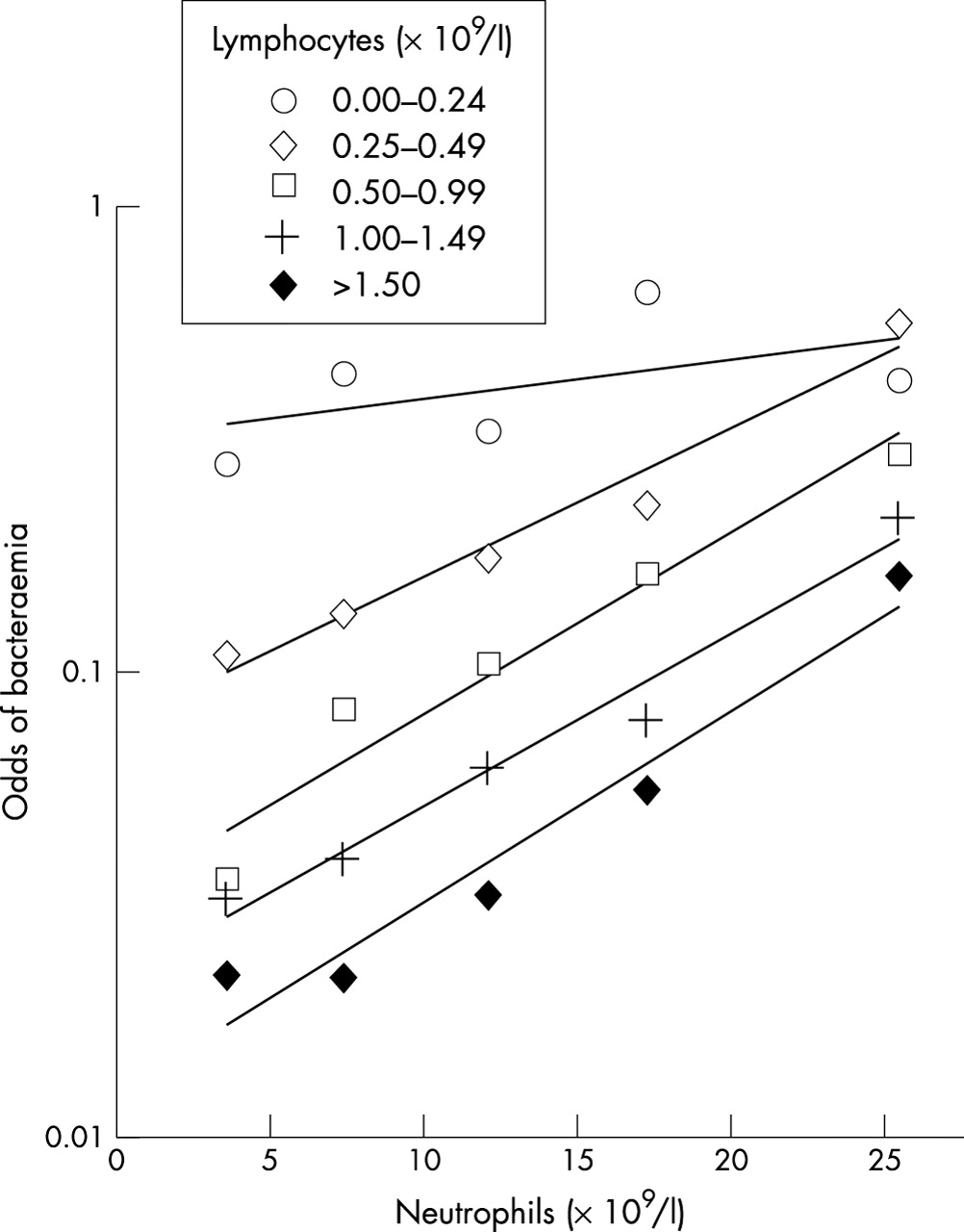
The observed odds of bacteraemia (the number of patients with bacteraemia/number without bacteraemia) were calculated for the 7182 patients whose blood had been cultured, stratified by lymphocyte and neutrophil count. Table 2 shows the absolute numbers of patients in each stratum. In fig 3, a surface is drawn through the observed bacteraemia odds. As expected, odds of bacteraemia increased with increasing neutrophil count. However, there was also a pronounced increase in bacteraemia odds as the lymphocyte count declined below 1.5 × 109/litre, an effect evident at all neutrophil counts. This suggests that neutrophilia and lymphopenia independently predict bacteraemia.
Distribution of lymphocytes and neutrophils in patients with medical emergencies

Odds of bacteraemia by cell count. The odds of bacteraemia (number of patients with bacteraemia/number without bacteraemia) among the patients whose blood was cultured, stratified by neutrophil and lymphocyte counts.
Lymphocyte counts less than 0.25 × 109/litre, referred to here as extreme lymphopenia, identified the group with the highest risk of bacteraemia. This is evident from fig 4, which shows an alternative representation of the data in fig 3. Extreme lymphopenia was found in 12% (63 of 530) of the patients with bacteraemia, but only 2.4% (162 of 6652) of the patients without significant isolates. Extreme lymphopenia, similar to less severe lymphopenia, appears to recover during hospital stay: the mean difference between admission and predischarge lymphocyte counts was 0.62 × 109/litre (95% confidence interval, 0.48 to 0.76) with extreme lymphopenia, and 0.36 × 109/litre (95% confidence interval, 0.29 to 0.43) without extreme lymphopenia.
Odds of bacteraemia by cell count. The odds of bacteraemia (number of patients with bacteraemia/number without bacteraemia) among the patients whose blood was cultured, stratified by neutrophil and lymphocyte counts. An alternative representation of the data in fig 3.
Interestingly, in the extreme lymphopenic group, the strength of the association of bacteraemia with the neutrophil count appears to be less than that at higher lymphocyte counts. Mathematically, this would represent an interaction between neutrophil and lymphocyte counts. To investigate this further, and to examine the effect of age, logistic regression was performed. Univariate logistic regression showed that the neutrophil count, the lymphocyte count, and their interaction were strongly associated, and age and WBC were weakly associated with bacteraemia (table 3). WBC was not used in multivariate modelling because of a strong correlation with neutrophil count. Of the other variables, neutrophil count, lymphocyte count, their interaction, but not age, remained significant on multivariate analysis (table 3).
Logistic regression relating significant bacteraemia to full blood count
Comparison of counts in bacteraemia prediction
Single variables associated with disease are simple to use clinically, and are potentially of diagnostic value. The 7182 blood cultured cases were examined, both as a whole, and in age stratified bands, and a comparison was made of the ability of raised WBC, depressed lymphocyte count, and raised neutrophil count to predict bacteraemia using ROC plotting. A significantly higher AUC, a parameter reflecting discriminatory ability, was found for lymphocyte count compared with either WBC or neutrophil count (fig 5). This effect was also evident in age stratified analysis; the lymphocyte count performed significantly better than the WBC or neutrophil count in all but one of the strata examined (table 4).
AUCs (95% CI) for the discrimination of patients with bacteraemia from those without bacteraemia

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
White cell count (WCC) components predicting bacteraemia. A receiver operator characteristic plot is shown, illustrating the ability of admission WCC, neutrophil count, and lymphocyte count to predict bacteraemia among all 7182 patients in whom blood cultures were taken. The symbols on the curve indicate the positions of particular counts; for example, the circle 1.0 indicates the performance of a lymphocyte count of 1.0 × 109/litre. Areas under the curve, and their confidence intervals (CI), are shown in the box for each variable. Higher areas under the curve indicate better discrimination.
DISCUSSION
Our study describes the quantitative association between lymphopenia and the risk of bacteraemia in a large cohort of patients admitted to a UK hospital with medical emergencies. Both lymphopenia and neutrophilia are independently associated with bacteraemia, and there is a group of patients who are lymphopenic, and at very high risk of bacteraemia, whose total WBC and neutrophil counts lie within the normal range. The lymphopenia–bacteraemia association was seen in patients at all ages studied.
Our observations are compatible with reports from smaller series of elderly patients describing lymphocyte counts less than 1 × 109/litre as being associated with bacteraemia.11,12 An association of bacteraemia and lymphopenia may also explain the associations between lymphopenia and disease severity in nursing home residents with pneumonia,9 and surgical patients after emergency laparotomy.15 Our observations are also compatible with the rapid decline in blood lymphocyte count occurring in animal and human models of sepsis.5–7 Bacterial sepsis was an important cause of lymphopenia in the population studied, but lymphopenia is not specific for sepsis of bacterial origin, because it also occurs in severe viral infections.16–18
Although the hospital in which the study was performed is a tertiary referral centre, the study cohort comprised individuals admitted from the community as an emergency. As such, they are likely to be representative of emergency medical admissions in the UK. Their microbiological investigation was probably typical of that widely practiced, because the proportion of patients cultured in this cohort was similar to that reported from a comparable cohort in another European hospital.12
HIV associated lymphopenia might complicate the observed association between lymphopenia and bacteraemia. However, HIV prevalence, determined by an unlinked seroprevalence study,19 was about 1/1000 during the study, and the lymphopenia–bacteraemia association was seen at all ages, including the elderly, in whom HIV is extremely rare in Oxfordshire,19 so HIV related changes in WBC are unlikely to be an important confounder.
We used a stringent definition of significant bacteraemia, regarding all isolates except Corynebacterium spp or coagulase negative staphylococci as significant for the purpose of our study. Therefore, our definition will classify many organisms, including α haemolytic streptococci and enterococci, as significant. Although such organisms are sometimes associated with serious pathology, their isolation may also be of little importance, especially when only isolated from a single culture. A chart review could have been used to determine the probable relevance of individual cases. However, this process is often subjective, so we persisted with a stringent definition, which probably led to an underestimation of the true lymphopenia–bacteraemia association.
“The clinical usefulness of lymphopenia as a diagnostic and prognostic marker merits further investigation in other centres and populations”
The induction of tumour necrosis factor family members occurs early in the inflammatory response; these engage receptors expressed on lymphocytes and cause lymphocyte apoptosis, as reviewed previously.20 The decline in lymphocyte numbers seen in our study is probably the result of large scale lymphocyte apoptosis, which has been seen in several animal models of sepsis,21,22 in the spleens of humans who have died of sepsis,23 and in the peripheral blood of patients with sepsis.6,23–25 Interestingly, CD4 T helper type 1 and 2 cells may be differentially susceptible.25,26 The study of mice with genetic abnormalities of the apoptotic machinery, and of mice treated with apoptosis inhibitors,27,28 shows that lymphocyte apoptosis influences mortality in sepsis. This is probably because protective lymphocyte dependent immune responses24 are decreased by the widespread death of lymphocytes. These studies imply that the decline in peripheral blood lymphocyte numbers seen in our study is the result of a key pathogenic mechanism in sepsis.
The data presented in our paper show that, in populations with a high prevalence of bacterial infections, lymphopenia may reflect bacteraemia. Importantly, in our large cohort, lymphopenia performed significantly better than either neutrophil count or WBC in bacteraemia prediction, although these last two markers are very widely used in the assessment of infected patients. Therefore, the clinical usefulness of lymphopenia as a diagnostic and prognostic marker merits further investigation in other centres and populations, both alone and in combination with other laboratory measures of the acute phase response.29,30
Take home messages
-
In a cohort of adult medical admissions with suspected bacteraemia, neutrophilia and lymphopenia were both associated with bacteraemia, although lymphopenia was the better predictor
-
Both neutrophilia and lymphopenia were more predictive of bacteraemia than the total white blood cell count
Acknowledgments
We thank Professor J Wainscoat and Drs A Berendt, N Day, P Klenerman, and E Torok for helpful comments.