Article Text

Statistics from Altmetric.com
A 65 year old man was brought into the resuscitation room in cardiac arrest. Forty five minutes earlier he had become short of breath before collapsing. The only other history available was that he had undergone a left pneumonectomy several years previously for carcinoma of the lung but was thought to have made a full recovery. Basic life support was performed by the patient's work colleagues and when the paramedics arrived the patient was asystolic. He was treated according to Advanced Life Support (ALS) guidelines1 and briefly regained a cardiac output before he arrested again, this time in electro-mechanical dissociation (EMD). A total of 8 mg of adrenaline (epinephrine) was given by the paramedics. On arrival at the accident and emergency department the patient was intubated and cannulated. The endotracheal tube position was checked and breath sounds were audible on both sides of the chest. There was little movement of the left side of the chest and the trachea was deviated towards that side; there were scars consistent with his previous surgery over the left chest wall. The right side of the chest was hyperexpanded.
The patient was in EMD and the ALS protocol was followed. Intravenous fluids were started and after two further 1 mg doses of adrenaline there was a return of spontaneous circulation. Chest radiography was performed. At this time there was no spontaneous respiration and the highest oxygen saturation recorded by pulse oximetry was 80%. The patient briefly arrested again (EMD) but responded to a single 1 mg bolus of adrenaline.
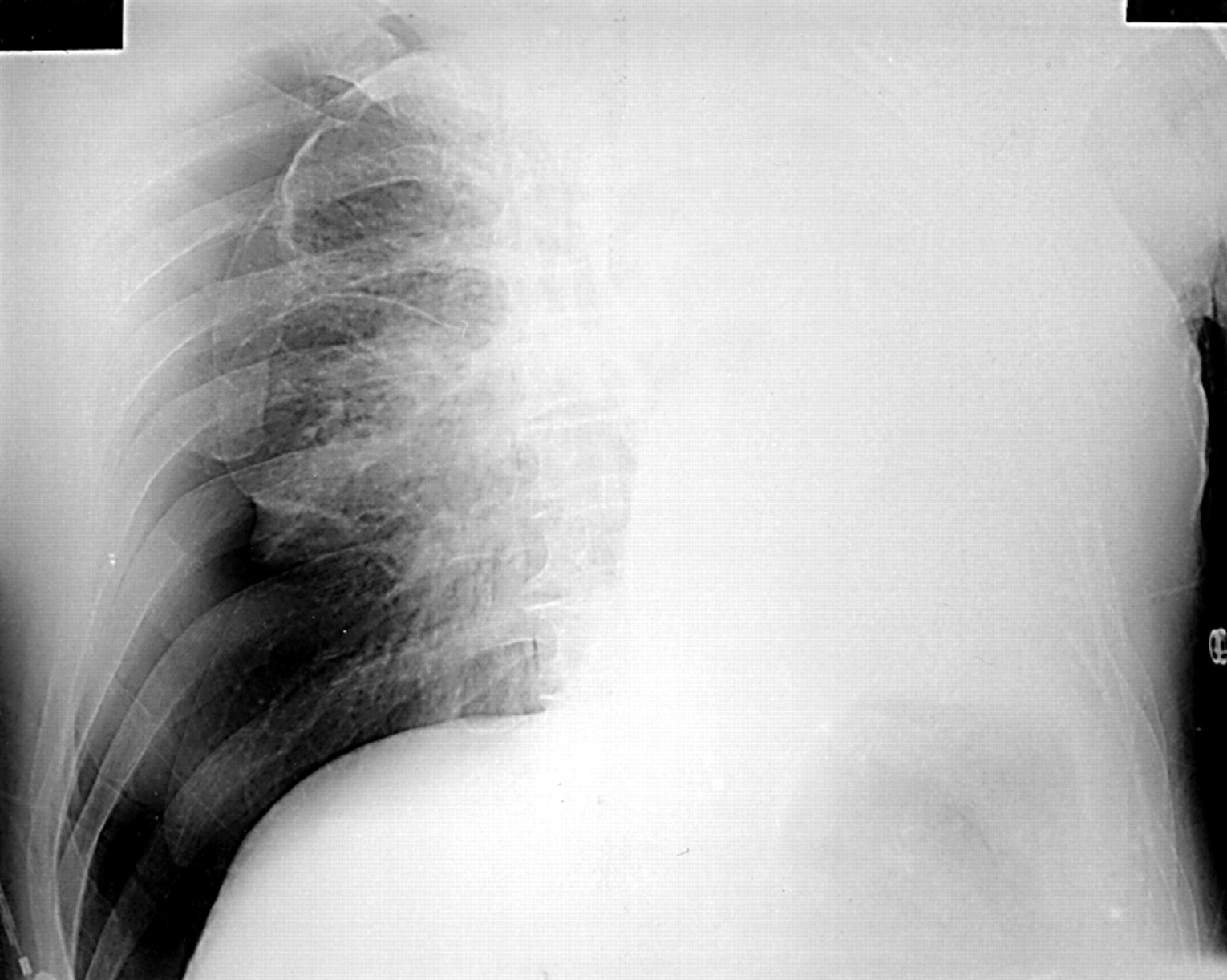
The chest radiograph showed a right sided pneumothorax (fig 1). A 14G intravenous cannula was inserted into the right second intercostal space in the mid-clavicular line and a clear “hiss” of air was heard as the needle was withdrawn. The patient's clinical condition immediately improved with oxygen saturation reading 99% on oxygen via the endotracheal tube. An intercostal tube was inserted (fig 2) and the patient was transferred to the intensive care unit where he unfortunately died approximately 30 hours after admission. A postmortem examination revealed that the cause of the right pneumothorax was a ruptured bulla; the cause of death was cerebral hypoxic damage.
A tension pneumothorax occurs when a one way valve is created between the lung and the pleura.2 This leads to an accumulation of air within the pleural cavity during each respiratory cycle, with a consequent increase in intrathoracic pressure. Eventually the ipsilateral lung collapses and the mediastinum is displaced away from the affected side. Venous return is impeded and cardiac arrest ensues. ALS teaches us to consider tension pneumothorax in patients who are in EMD cardiac arrest and to seek the classic findings of a deviated trachea and reduced breath sounds in such patients. In our patient the trachea was deviated to the left and the right side of the chest was hyperexpanded but these clinical findings were anticipated and thought to be secondary to his pneumonectomy. Breath sounds were audible bilaterally, presumably because of some residual lung tissue on the left side. It was not until the chest radiograph became available that the diagnosis of a right pneumothorax was realised. Although the deviated trachea and mediastinal shift were again probably secondary to pneumonectomy (these features remained on the post-intercostal drain), the patient's clinical condition suggested that the pneumothorax was under tension and this was confirmed by needle thoracostomy. This is clearly a very unusual situation but serves to remind us that previous pneumonectomy does not preclude a tension pneumothorax on the opposite side of the chest. Finally, if such a diagnosis is considered, the correct course of action is immediate decompression before obtaining radiological confirmation.

Chest radiograph showing a right sided pneumothorax and mediastinum shifted towards the left. There is a “white out” of the left lung field.

{kind=link}
{kind=link}
Chest radiograph after intercostal drain insertion showing the reinflated right lung. The mediastinum remains shifted towards the left.