Article Text

Statistics from Altmetric.com
- A&E, accident and emergency
- BASICS, British Association for Immediate Care
- CCT, Certificate of Completion of Training
- DoH, Department of Health
- GP, general practitioner
- GPwSI, General Practitioner with Specialist Interest (GPwSI)
- JCPTGP, Joint Committee on Postgraduate Training in General Practice
- PHEC, Pre-hospital Emergency Care
- PMETB, Postgraduate Medical Education and Training Board
- STA, Specialist Training Authority
The provision of on scene medical support to ambulance services in the UK is fragmented, disorganised, and largely unregulated. Recent and evolving educational, professional, and regulatory developments in medical practice now provide an opportunity to remedy this situation and ensure that “immediate care” is governed and regulated in the same way as any other specialist undertaking within the NHS.
Immediate care has been defined as the provision of skilled medical help at the scene of an accident or medical emergency and during transportation to hospital.1 Well before the development of modern ambulance services and the recognition of accident and emergency (A&E) medicine as a specialty, general practitioners (GPs) were required to deal with increasing numbers of critically injured patients in the pre-hospital environment. Their response, in most parts of the UK, was to form themselves into voluntary associations and create a framework within which their training, equipment, and operational activity could be organised and funded.1–3 These “immediate care schemes”, in stark contrast to the systems developed in the United States and elsewhere in Europe, were, and still are, funded almost entirely through charitable donations.
In some parts of the country, hospital practitioners have also played a role in the provision of immediate care, either through “flying squads” or mobile medical teams or by individual membership of immediate care schemes.2,3 Some hospitals continue to deploy mobile teams at the request of ambulance services. Unfortunately, the provision of such services continues to be unpredictable, and there are very wide variations in availability, funding, training, experience, and equipment.4–6 There also appears to be considerable uncertainty regarding the composition, training, and role of hospital mobile medical teams in incidents that are not declared as major incidents.
Regardless of their background, the core activities that define the clinical practice of immediate care have remained essentially unchanged over the last 40 years. They can be defined by scrutinising the activity of individual schemes and doctors and ambulance service medical advisors and directors.2,7,8,9,10,11 In our experience, this practice includes direct clinical care at the scene and during retrieval to hospital (in transit care), scene management, major incident management, clinical leadership (for example, medical director functions) and supporting professional activities such as training and education of ambulance service personnel.
Doctors involved with immediate care have historically undertaken a spectrum of activities from simple first aid and basic resuscitation to high stakes critical care interventions. The development of modern ambulance services has further polarised this activity. At one end of the spectrum, there clearly remains a need for basic first response capabilities in rural areas. This has been recognised through initiatives such as the NHS Scotland Remote and Rural Areas Resource Initiative (which provides funding for standardised training for remote and rural medical practitioners)12 and immediate care scheme involvement in development of community based lay response systems. At the other end of the spectrum, there also remains a need for specialist on scene and in transit medical support. The most common examples in our experience are the patient with immediately life threatening asthma and respiratory failure who is remote from hospital, and the seriously injured vehicle occupant who is trapped at the scene. The relative infrequency of such patients does not diminish their critical care needs or the impact that they have on NHS resources. There seems little doubt that the timely intervention of a competent specialist with the full range of critical care skills can have a major impact on such a patient’s journey, in terms of early diagnosis, meaningful interventions, triage, or advocacy.13–16 The care of such patients often requires difficult clinical decisions that are likely to remain beyond the scope of most healthcare professionals employed by ambulance services for the foreseeable future.17–20 We would argue that many of these decisions and interventions are likely to also be beyond the scope of the “occasional” or “fringe” immediate care doctor.
Given the emergence of “intermediate” care and confusion surrounding the medical practitioner’s contribution to pre-hospital care, we propose that the term “pre-hospital and retrieval medicine” be used as a more accurate description of this area of specialist practice. In our current practice, we frequently attend incidents in rural areas, provide on scene medical care, undertake procedural sedation or emergency anaesthesia at the scene, and take responsibility for in transit medical care for 30–60 minutes. We believe that this represents a specialist function within the Ambulance Service spectrum of activity. The concept of “pre-hospital and retrieval medicine” being considered as a specialist endeavour rather than an occasional pursuit is not new.1,21,22 The glaring inconsistency between the requirement for a predominantly consultant led emergency department phase compared to a paramedic or technician led pre-hospital phase for the same critically ill or injured patient is now, however, more difficult to defend other than on historical grounds. It is clearly recognised that time to meaningful intervention related to injury pattern is probably the most important determinant of survival following traumatic injury.23–25 There is no doubt that short scene times and rapid transfer to the appropriately staffed and prepared hospital should be the norm for most patients, but what of those who cannot be transported (entrapment) or who have urgent pre-hospital critical care needs that cannot be met from current paramedic or emergency care practitioner education and training? In addition, trauma care systems are changing, with the recognition that a balance has to be struck between local hospital access and the concentration of multispecialist expertise in regional centres.26 A regional trauma system further increases the need for on scene medical care, selection of the most appropriate facility to meet each patient’s needs, and safe retrieval to that facility. There is currently no system, training stream, or workforce in place across the UK to ensure that the needs of these patients are met in a consistent or organised manner.
BASICS
The British Association for Immediate Care (BASICS) was formed in 1977 with the aim of becoming the national co-ordinating body for those providing immediate care throughout the UK. It has been instrumental in the development of the Resuscitation Council, the Diploma in Immediate Medical Care (Dip IMC) and the Faculty of Pre-hospital Care of the Royal College of Surgeons of Edinburgh.3 In 1998, BASICS introduced a voluntary accreditation scheme for its members. However, uptake has been poor, and few ambulance services or immediate care schemes have sought to enforce or even apply the BASICS accreditation standards to doctors who deliver a clinical service (box 1). Organisations that employ doctors, such as the London Helicopter Emergency Medical Service (HEMS) and Great North Air Ambulance (GNAS), do not require applicants to hold and/or maintain BASICS accreditation. Similarly, A&E departments who routinely send doctors to incident scenes do not require them to be BASICS accredited. The accreditation standards themselves are also widely regarded as primarily aimed at the occasional practitioner in rural areas (for example, completion of a 3 day Pre-Hospital Emergency Care (PHEC) course). Those organisations that have applied standards tend to use the Dip IMC as a benchmark. This has been recommended as the minimum qualification for doctors regularly called out by ambulance services by both BASICS and the Royal College of Surgeons.1,26,27 Despite this, the Dip IMC is not a minimum requirement for BASICS accreditation and it has not become a mandated prerequisite for operational activity supporting ambulance services.
Box 1 BASICS Accreditation Requirements for Doctors (from www.basics.org.uk)
-
Full GMC registration
-
Evidence of professional development in the field of pre-hospital care
-
PHEC certificate or Immediate Care Course or Dip IMC or FIMC
-
Evidence of operational activity in the pre-hospital environment
-
Recommendation from an accredited BASICS member
-
Indemnity insurance is provided for
-
Individual member of BASICS
-
Undertaking to agree to BASICS accreditation requirements/code of practice
THE FACULTY OF PRE-HOSPITAL CARE
The Dip IMC is administered by the Royal College of Surgeons of Edinburgh and its Faculty of Pre-hospital Care. The faculty was formed in 1996 with the central aim of setting and maintaining standards of practice in pre-hospital care. The Dip IMC has undergone extensive development and is now open to nursing and paramedic professionals. Paradoxically, the current regulations for the Dip IMC require “documented evidence of clinical experience in the area of pre-hospital emergency care for a period of 1 year”.28 Perhaps as a result of this perceived restriction, a wide range of short vocational courses such as PHEC, Pre-hospital Trauma Life Support (PHTLS),29 Pre-hospital Paediatric Life Support,30 Safety at Scene,31 and Major Incident Medical Management and Support32 have become regarded as sufficient in themselves to qualify or accredit doctors for practice in pre-hospital care.
A new Fellowship examination has recently been created, which is only open to doctors who have obtained the Dip IMC or its equivalent and have at least 4 years’ post-registration experience. It could therefore be taken 2 years after the Dip IMC. The concept of the FIMC as a specialist exit examination is implicit in the regulations and reflects the level of expertise and competence required for specialist practice. The regulations state that experience must be in the “specialist area of immediate medical care” and that the examination is “only open to those who have undertaken and successfully completed a training programme approved by the Specialty Advisory Board”.28 These examination developments mirror, to some degree, the rigour applied to the Examination of Special Competence in Emergency Medicine of The College of Family Physicians of Canada,33 the Postgraduate Diploma in Community Emergency Medicine in New Zealand34 and the Diploma in Primary Emergency Care of the College of Family Practitioners of South Africa.35 There is, however, no formally constituted or recognised training programme in immediate care in the UK.
THE NEW GP CONTRACT
In addition to the work of BASICS and the Faculty of Pre-hospital Care, the new GP contract adds weight to the argument for recognition of pre-hospital and retrieval medicine as a subspecialty activity undertaken only by those who are recognised as competent to do so. The contract has made provision for primary care organisations (PCOs) and GPs to contract for enhanced services to meet local health needs. These enhanced services can include specialist interests in addition to the essential traditional GP services. The contract documentation includes a detailed national enhanced service (NES) specification for “provision of immediate care and first response care” (box 2).36 Although the NES represents an important step in recognising the role of General Practice in provision of immediate care, it does not differentiate first response services from more specialist pre-hospital critical care. The specification does, however, make explicit the need for GPs to demonstrate competence. It states (under the heading “accreditation”) that GPs must satisfy at appraisal and revalidation that they have the relevant “continuing medical experience, training, and competence as is necessary for them to be able to contract for the enhanced service”. The specification goes on to state that GPs should, as a minimum, have completed the PHEC course or its equivalent. The role of BASICS and the Faculty of Pre-hospital Care as the standard setting and accreditation bodies is also endorsed.
Box 2 NES accreditation standard for provision of immediate and first response care (from reference 36)
Practitioners will normally be expected to:
-
as a minimum, possess the Pre-Hospital Emergency Care (PHEC) Certificate of the Royal College of Surgeons of Edinburgh or other equivalent pre-hospital emergency medicine qualification;
-
undertake a local orientation and familiarisation programme;
-
undergo such advanced driving tuition as required by the Ambulance Service;
-
undertake such communications systems training as required locally;
-
undertake such refresher training as dictated by good clinical governance and the need to remain accredited;
-
accept and obey the local statutory emergency service command structures;
-
if the NES is operated locally through a local immediate care scheme, accept its rules and operational standards;
-
maintain appropriate communications with the tasking control room concerning personal availability for call out;
-
be familiar with the scope and limitations of paramedic practice;
-
be willing to work in a team;
-
accept the ambulance service tasking policy.
Practices or individuals that are contracted to provide such services should be able to demonstrate competencies in all the above areas, and in addition should be able to show active participation in service development through CPD, audit, and critical case analysis. The keeping of an individual log of incidents attended and interventions is mandatory. Accreditation may be achieved by meeting the standards set by a mutually agreed third party such as a local immediate care scheme, British Association for Immediate Care, or the Faculty of Pre-Hospital Care. This should occur on an annual basis and be summarised in an annual report. Such professional organisations should be asked to review a doctor’s performance if there is any doubt or dispute over an individual’s or practice’s status.
GENERAL PRACTITIONERS WITH SPECIAL INTERESTS
In a parallel development, the Department of Health (DoH) General Practitioner with Specialist Interest (GPwSI) project has encouraged PCOs to support GPs and allied health professionals who wish to develop specialist interests and expertise in particular clinical areas. While this development has been primarily aimed at improving access to outpatient services (for example, ear, nose and throat), the DoH has commissioned the Royal College of General Practitioners (RCGP) to develop a framework for GPwSI appointments in “Emergency and Unscheduled Care”.36,37 This framework includes pre-hospital and “scene of incident” care, and explicitly states that a process of accreditation should be undertaken by the “employer” organisation (acute trust, ambulance trust, or PCO). This accreditation process should be related to evidence of having achieved an agreed and defined set of competencies (although it is recognised that the competencies themselves have not been defined). The framework documents go on to state that “a diploma or similar formal qualification can provide a credible source of evidence of the acquisition of the required competencies”. The PHEC is described as an example of an “entry level” course.37
The GPwSI framework provides a much more robust mechanism for accreditation, appointment, and funding of appropriately trained specialist medical support to ambulance services than the NES provisions within the new GP contract. Applicants for such posts must show proof of competency as a GP and provide evidence of competence in the special interest area sufficient to meet the requirements of the post.38 This mirrors established arrangements for hospital subspecialty recognition: evidence of competency in the subspecialty is required in addition to proof of competence as a consultant within a defined specialist area. Although the NES funding arrangements could be applied to a GPwSI, the NES specification is perhaps better suited to GPs contracted to provide first response services.
LICENSING AND REVALIDATION
Additional recent developments within medical regulation provide further impetus for development of pre-hospital and retrieval medicine as a recognised subspecialty of both general and hospital practice. From 2005, all doctors who wish to practice medicine in the UK will be required to hold a license to practice in addition to their registration. Although rarely explicitly stated, we believe that this license will be specialty specific. Central to the award of a license are the training and revalidation processes. The evidence required to show compliance with the principles of good clinical care (the first of the seven attributes of good medical practice examined by revalidation) is, by definition, speciality specific.39 Thus, if pre-hospital and retrieval medicine was recognised as a specialist endeavour, neither a GP or a consultant in emergency medicine would have a license to practice in this area unless they could demonstrate achievement and maintenance of professional competence. Recognition of pre-hospital and retrieval medicine as a specialist endeavour will ensure that critically ill and injured patients obtain the same regulatory protection in the pre-hospital environment as they would in any other healthcare setting.
REFORM OF POSTGRADUATE MEDICAL EDUCATION
The drive for the development of an NHS workforce that is fit for purpose has led to fundamental reform of both undergraduate and postgraduate medical education and training.40 All medical graduates of the future will complete a 2 year Foundation Programme, which will provide the appropriate background for entry into specialist and general practice training. On completion of this programme, doctors will be able to apply directly to competency based specialist or general practice training programmes within recognised training rotations, which will lead to a Certificate of Completion of Training (CCT). The existing Specialist Training Authority (STA) will be absorbed into the new Postgraduate Medical Education and Training Board (PMETB). For General Practitioners, it is intended that the Joint Committee on Postgraduate Training in General Practice (JCPTGP), the current equivalent of the STA, also becomes absorbed into the PMETB. The PMETB will therefore become the UK competent authority for accreditation of both general and specialist practitioner training.
There are currently 55 recognised medical specialties and 29 subspecialties. We understand that an NHS consultant’s license to practice will be directly related to their recognised specialist and subspecialist accreditation on the GMC Specialist Register. Within the specialty of accident and emergency medicine, paediatric accident and emergency medicine is the only currently recognised subspecialty. The process for recognition of a new subspeciality in pre-hospital and retrieval medicine is likely to be similar to the existing arrangements.41 The PMETB will require a competency based curriculum, framework and training programme that meets its standards (box 3) and that has been agreed between the Faculty of Pre-hospital Care, the Faculty of Accident and Emergency Medicine, the RCGP, and BASICS.42 There is no reason why such subspecialty recognition, leading to a license to practice, cannot be included on the proposed General Practice Register in much the same way as for a consultant on the Specialist Register.
Box 3 Key Principles and standards for postgraduate medical education training programmes (Adapted from reference 40)
The programme must:
-
have defined, patient centred, learning outcomes; be developed jointly with the disciplines concerned, the trainees, patients, public and the service;
-
be based on the standards of professional practice set out in Good Medical Practice;
-
include any generic learning outcomes required by the PMETB;
-
have explicit, published entry criteria and selection processes that are valid, reliable, open and comply with current equal opportunities legislation;
-
have arrangements to support trainees to train and work flexibly;
-
have arrangements to support trainees who have special needs;
-
be designed to support the needs of doctors who may enter training at a number of different levels with varying levels of knowledge and skills;
-
have processes in place for the regular evaluation and review of the programme and its outputs;
-
have processes for ensuring that trainees provide information on their supervision, training and clinical experience.
The curriculum must:
-
include details of the intended learning outcomes and a syllabus of knowledge, skills, and professional attitudes and behaviours;
-
allow training and learning to be delivered flexibly in ways that are relevant and meet trainees’ learning needs;
-
provide experiential learning through systematic clinical training;
-
involve trainees in the supervised delivery of service;
-
provide for regular formal educational sessions that cover topics of value and topics of interest to trainees;
-
include a systematic programme of valid and reliable formative and summative assessments;
-
provide opportunities and processes for self-directed learning, regular feedback, career advice and counselling, extra support, and remediation and retraining.
Those responsible for programmes must ensure that:
-
there is a clear statement of responsibility for the different aspects of the programme;
-
those who have responsibilities for teaching have the skills, attitudes and practices of a competent teacher and that trainees are properly supervised;
-
there are sufficient resources to achieve the programme’s learning outcomes;
-
there are sufficient resources in the trust, primary care organisation, practice or other organisations where the trainee is being placed to allow the training to be undertaken effectively;
-
there is provision of adequate resources to support trainees personal learning needs;
-
they have an appropriate working knowledge and understanding of the regulatory framework in the UK.
A POSSIBLE ROUTE TO SUBSPECIALTY ACCREDITATION
Doctors who wished to develop a subspecialty practice in pre-hospital and retrieval medicine would be required to undertake a training programme recognised by the PMETB (fig 1). Entry to the programme might follow the model and procedures proposed for competitive entry to general and specialist training programmes.40 The Dip IMC has been widely and repeatedly advocated as an appropriate benchmark for immediate care practitioners and it, or its equivalent, should also therefore be a pre-requisite for entry to any training programme. Given the need to have some pre-hospital emergency care experience prior to attempting the Dip IMC, an entry level vocational course such as PHEC or those delivered by BASICS Scotland could remain the minimum recommended basic training prior to undertaking supervised clinical experience. Unsupervised clinical duties at this stage should be no more encouraged in pre-hospital care than they are currently in general or specialist practice.

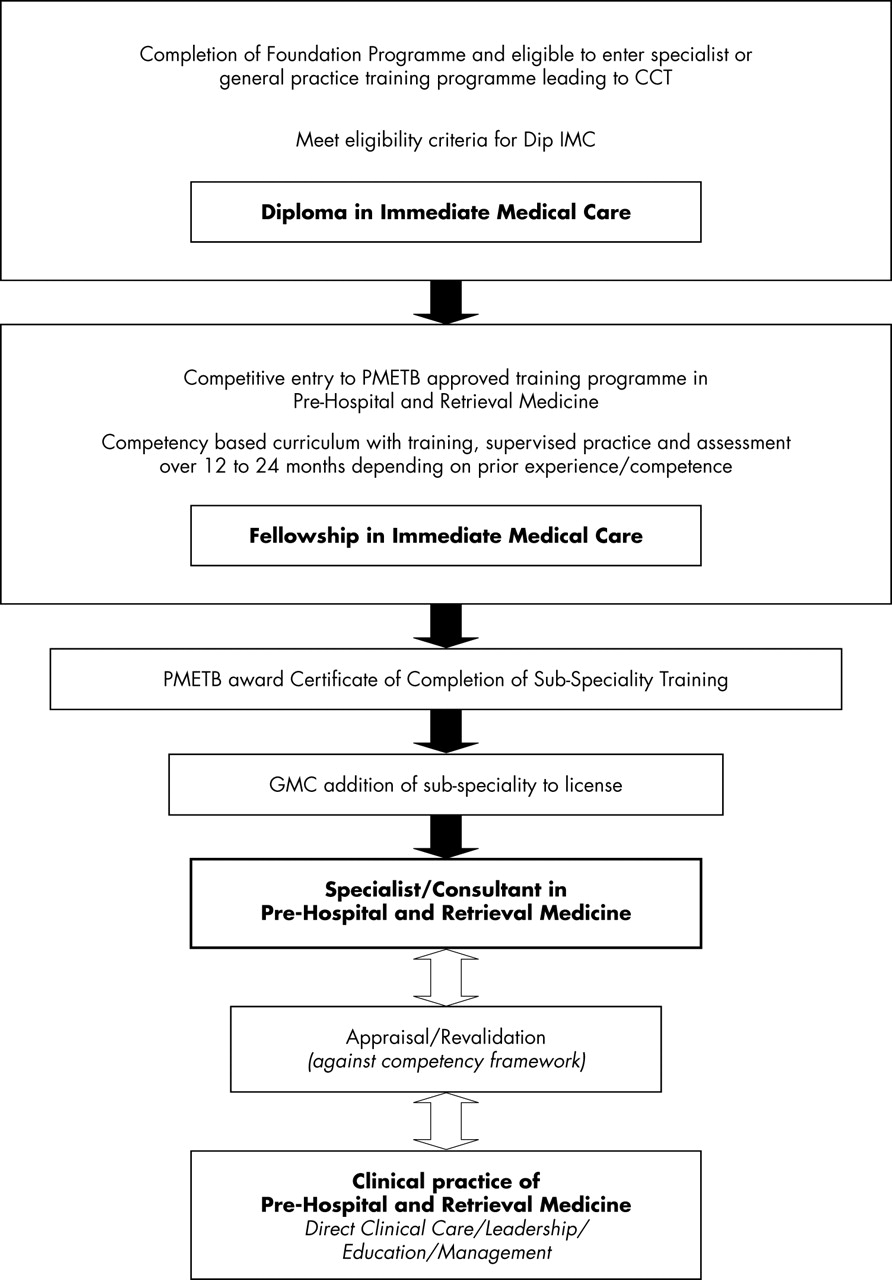{kind=link}
A framework for subspeciality training and registration for pre-hospital and retrieval medicine.
Once accepted onto a training programme, the doctor could be required to register with a professional body such as the Faculty of Pre-hospital Care in order to undertake a review of their training and experience against a clearly defined competency framework. A tailored programme of training and supervised experience lasting 12–24 months would then be agreed and progress through the programme monitored. Towards the end of the training programme, the doctor could be required to complete the FIMC. On completion of the training programme and the exit examination, representation would then be made to the PMETB for recognition of subspecialty training. This may need to be linked to the underpinning CST in specialist or general practice but it is not clear whether this would be necessary in reality as some doctors may have further training to complete before the award of a CCT.
Development of a subspecialist interest in pre-hospital and retrieval medicine would not be restricted to those at the beginning of their medical careers. A fundamental tenet of Modernising Medical Careers is that systems should be in place to allow entry to recognised training programmes by doctors at various stages in their careers.40 In addition, a pre-hospital and retrieval medicine training programme need not be a full time endeavour and some flexibility would need to be applied by the professional body (e.g. the Faculty of Pre-hospital Care) to ensure that prior learning and sessional, part-time and voluntary experience can all be incorporated into training programmes. This mirrors the approach taken by the Faculty of Accident and Emergency Medicine, which already recognises some pre-hospital activities for A&E training (e.g. within the military, with London HEMS and within some immediate care schemes).
COMPETENCY DRIVEN TRAINING AND ASSESSMENT
Central to the concept of subspecialist accreditation and practice is a competency based programme with relevant training, assessment and supervised practice.40–42 In developing such programmes, there is a critical distinction to be made between the rural practitioner who has occasional need to support the ambulance service as a first responder (with skills equivalent to a modern paramedic) and the specialist practitioner who is engaged or employed by ambulance services specifically for the purposes of providing specialist on scene, special incident, and major incident medical support. The scope of clinical practice has been mentioned above and is neatly delineated by the 10 core competency themes in the current training programme utilised by Cambridgeshire’s immediate care scheme, MAGPAS (box 4).43 Work is currently underway to develop these themes into a competency based curriculum and syllabus of knowledge, skills, and professional attitudes and behaviours.
BOX 4 The 10 themes in the MAGPAS competency framework for specialist training in Pre-hospital and Retrieval Medicine
-
Operational environment
-
Resuscitation and clinical care
-
Equipment and monitoring
-
Care of children
-
Rescue and extrication
-
Analgesia and procedural sedation
-
Pre-hospital emergency anaesthesia
-
Special incident medical support
-
Major incident medical support
-
Retrieval and transfer
We believe that there is an opportunity for the Faculty of Pre-hospital Care to set and maintain the standards for both training and assessment for such a programme, building on its existing work with accreditation, the Dip IMC and the FIMC. Monitoring and evaluating the delivery of training would also become the remit of the PMETB. Actual delivery of training should probably remain a core activity of BASICS and BASICS Scotland together with ambulance trusts, universities, immediate care schemes and other faculty accredited course providers.
With regard to supervised practice, a number of models currently exist in the UK, which are well established in terms of organisation, training, and supervision and which could be adapted to meet the needs of such a training programme. Examples of these currently include helicopter based services such as the Teeside based Great North Air Ambulance (www.greatnorthairambulance.co.uk) and London HEMS (www.hems-london.org.uk) as well as land based services such as the MAGPAS Emergency Medical Team (www.magpas.org.uk) and the West Midlands CARE Team (www.wmcareteam.com).
A CALL FOR ACTION
Reform of emergency care has encouraged radical thinking and innovative practices across the spectrum of emergency, unscheduled, and out of hours care demands. A new generation of healthcare professionals are being given the education, training, and confidence to address many of these demands. Among all this change, however, there is a tendency to underestimate the needs of critically ill or injured patients in the pre-hospital phase and undervalue the role of an appropriately trained and equipped physician in their management. The daily operational activity of volunteer immediate care doctors around the UK and their heavy involvement in ambulance service development serves to remind us of the continued need for access to such physicians in the “therapeutic vacuum” between injury or illness and meaningful intervention. Although the language and terminology differ, developments within BASICS, the Faculty of Pre-hospital Care, the RCGP, the DoH, and the GMC reveal a clear recognition of the need for competence and professional regulation in delivery of specialist pre-hospital care.
Patients have a right to expect that the same standards of professional medical regulation will apply in the pre-hospital phase of their journey as in the hospital phase. There are now opportunities to develop a framework for a properly trained and regulated medical workforce capable of providing specialist medical support to ambulance services. The development of a rigorous, accredited career stream in pre-hospital and retrieval medicine would fill one of the few remaining gaps in the provision of emergency care in the UK. There is real opportunity for both individual practitioners and the organisations responsible for regulating and applying standards to now collaborate and reach agreement on the scope of practice, competency framework and licensing arrangements for the subspecialty of pre-hospital and retrieval medicine.
Acknowledgments
This work was supported by funds from the MAGPAS Research Programme.
REFERENCES
Footnotes
-
Competing interests: R Mackenzie is a member of BASICS and the Faculty of Pre-hospital Care of the Royal College of Surgeons of Edinburgh. He is also an examiner for the Dip IMC and the Deputy Associate Editor for Pre-hospital Care for the EMJ. D Bevan is a member of BASICS. the opinions expressed are those of the authors and not of either the Faculty of Pre-hospital Care or BASICS.
Linked Articles
- Primary Survey