Article Text

Statistics from Altmetric.com
The assessment and management of neurological symptoms presents a particular challenge in the community, as the differential diagnosis may be wide and include potentially serious conditions. Whilst the practitioner may commonly encounter conditions such as stroke and the fitting patient, all patients will require careful assessment to avoid the pitfalls of missing a serious underlying diagnosis. Headache presents a particular diagnostic difficulty where the cause may range from the benign, to the life-threatening subarachnoid haemorrhage. Some neurological symptoms may be non-specific but indicate the possibility of rare conditions requiring urgent investigation and treatment. This first article will cover the primary survey positive patient including the unconscious patient, the fitting patient, and those patients presenting with headache as their main symptom. The second article will cover frequently encountered neurological symptoms and signs to enable the practitioner to develop a safe and comprehensive system to decide which patients need immediate treatment and/or referral and which may safely be treated at home.
THE PRIMARY SURVEY POSITIVE PATIENT
All patients should be assessed according to ABC principles in order to identify any immediately life-threatening conditions.
Box 1 Primary survey
If any observations below present treat immediately and transfer to hospital
-
Airway Obstruction
-
Respiratory rate <10 or >29 per minute
-
O2 sats <93%
-
Pulse <50 or >120
-
Systolic BP <90 mmHg
-
GCS <12
Neurological conditions can be immediately life threatening by causing an ABC problem:
-
Airway obstruction/compromise – loss of protective airway reflexes due to coma.
-
Breathing difficulty/inadequacy – apnoea due to conditions affecting the respiratory centre–for example, brainstem stroke, intracerebral haemorrhage; respiratory muscle weakness–for example, Guillain Barre, myasthenia gravis
-
Circulatory compromise – septic shock secondary to CNS infection, hypertension, and bradycardia in patients at imminent risk of coning.
The two main categories of immediately primary survey positive patients seen by the community practitioner are the unconscious patient and the fitting patient.
THE UNCONSCIOUS PATIENT
The unconscious patient is traditionally defined as having a GCS of 8 or less. It is very difficult to make an accurate neurological assessment of these patients and they will require a full hospital assessment. Arrange a 999 paramedic ambulance to transfer these patients to hospital.
Priorities in management will follow ABC principles well described elsewhere in this series.
Airway
Ensure an adequate airway using routine airway opening manoeuvres augmented by an oropharyngeal or nasopharyngal airway as appropriate. If there is any possibility of trauma then use a jaw thrust not a chin-lift, head-tilt. Give oxygen (15 litres via a non-rebreathing mask).
Breathing
Check the patient is breathing adequately. Hypoventilation will require bag/valve mask assistance. Check oxygen saturation by pulse oximetry.
Circulation
Check the pulse and if possible the blood pressure. Establish in vitro access if possible.
Disability
Measure the Glasgow Coma Score (GCS). If there is no response to pain check the tone in the limbs. When communicating the GCS score to secondary care it can be very usefully broken down into its separate components to give a clear impression of neurological status (Box 2). Check pupil size and reaction. A unilaterally dilated pupil may indicate an intracerebral heamatoma, pinpoint pupils may indicate a pontine stroke or raise the suspicion of poisoning–for example, opiates. Bilateral dilated pupils may suggest poisoning with benzodiazepines or tricyclic antidepressants.
Box 2 Glasgow Coma Score
Maximum Score = 15
Minimum Score = 3
A patient is defined as unconscious with a score of 8 or less
Eye response
4 Open spontaneously
3 Open to command
2 Open to pain
1 No eye opening
Verbal response
5 Fluent and orientated
4 Confused speech
3 Inappropriate words
2 Incomprehensible sounds
1 No verbal response
Motor response
6 Obeys commands
5 Localising pain
4 Withdraws from pain
3 Flexion to pain
2 Extension to pain
1 No motor response
In addition to ABCD, E (exposure) and G (glucose) should be assessed to search for clues as to the possible underlying cause eg. a rash may suggest meningitis or septicaemia (fig 1), puncture marks may indicate a drug overdose (fig 2).

Purpuric rash in meningococcal septicaemia.

Needletrack marks in intravenous drug user.
History
Try to gain as much information as possible to suggest possible causes of unconsciousness. Obtain a history of the episode from any witnesses; ask if they know of any previous medical history, prescribed medications, or history of illicit drug use. The main causes of unconsciousness are summarised in table 1.
Common causes of unconsciousness
Treatment
Treatment will be mainly supportive pending transfer to hospital. If a treatable cause is identified then this should be treated as soon as possible in order to minimise secondary brain injury. Hypoglycaemia should be treated immediately by either 10% glucose in vitro or intramuscularly glucagon administration. If there is strong suspicion that a patient may have taken an overdose of opiates and they have respiratory compromise, then intravenous or intramuscularly naloxone should be administered. If meningococcal disease is suspected then antibiotics should be given immediately (fig 3).
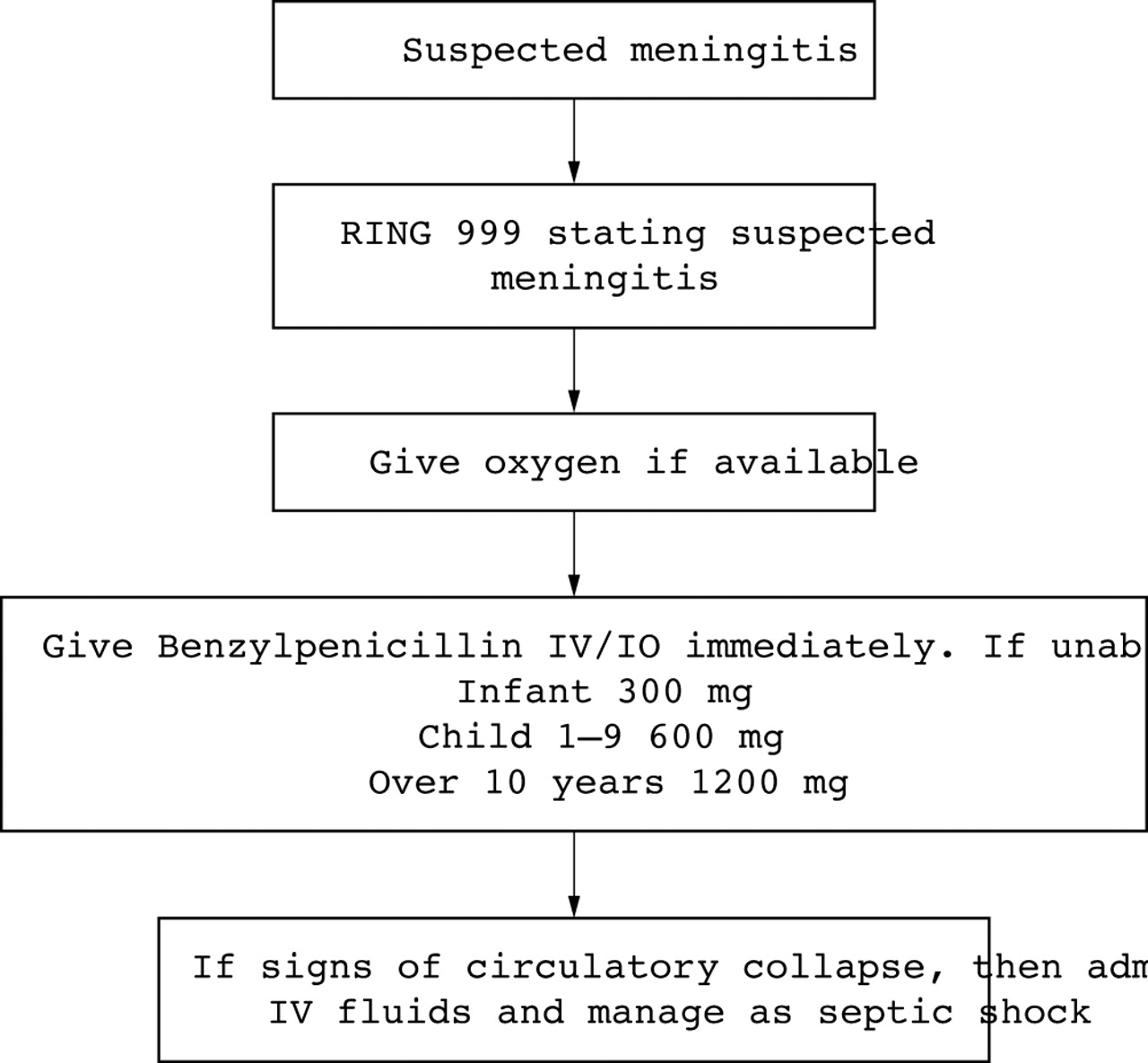
Treatment of suspected meningitis in the community.
THE FITTING PATIENT
The fitting patient can present a significant challenge to the practitioner. Attempts should be made to stop the fitting and assess further as required. The National Institute for Clinical Excellence (NICE) guidelines should be followed (Box 3).1
Box 3 NICE Guidance on fit management
If convulsive seizures lasting 5 minutes or longer or three or more seizures in an hour
-
Secure the airway
-
Assess respiratory and cardiac function
-
Give rectal diazepam in most cases with buccal midazolam an alternative
-
Call emergency services if required by the situation or the response to treatment, and particularly if
– Seizures develop into status epilepticus
– There is a high risk of recurrence
– This is the first episode
– There may be difficulties monitoring the persons condition
Airway management
Airway management in the fitting patient can be problematic due to jaw spasm, and a nasopharyngeal airway can be very useful if the fit is protracted with worsening airway compromise. Give oxygen and suction away any excess secretions. If possible place the patient on their side. Most fits will stop spontaneously. Do not forget to check the blood glucose.
If the fit is prolonged or recurrent, drug treatment may be required. Rectal diazepam is effective but it may be difficult to administer by a practitioner with no help. Intravenous diazemuls, lorazepam, or buccal midazolam are alternatives that may be used in accordance with local protocols.
Following cessation of the fit assess the patient for any obvious precipitating cause and for any injuries they may have sustained during the course of the fit. Common causes of fits are summarised in table 2. In patients with known epilepsy, fits may be precipitated by concurrent illness or changes in their medication. Injuries may include head and facial trauma, fractures, and burns. Rarely patients may sustain a posterior shoulder dislocation therefore shoulder movement should be checked.
Causes of fits
If the patient is a known epileptic, has a single fit and has completely recovered with normal vital signs and normal neurological examination, they may be safely left at home as long as there is family or carer support. If there is no previous history of fits, if the fit was unusual in any way, if there are abnormal examination findings or if there is concern about a possible precipitating cause, then the patient should be transferred to hospital for a full assessment.
Febrile seizures
A febrile seizure is any seizure occurring in an infant or young child (6 months to 5 years old) in conjunction with a fever or history a recent fever and without evidence of a previous febrile seizure or an underlying cause such as neurological disease or CNS infection. They are the most common seizures seen in the paediatric population in the prehospital setting, occurring in 2–5% of all children between the ages of 6 months and 5 years, therefore it is important that practitioners are familiar with the principles of their evaluation and management.2 Febrile seizures generally have a benign prognosis, however, dealing with these cases may be difficult as the parents are often upset and frightened by the seizure and require a calm, reassuring approach by the practitioner. The majority of these patients will have stopped fitting on arrival of assistance and most patients will only require minimal airway support during the post ictal period. Check oxygen saturations and circulatory status. Do not forget to check the blood glucose. It is important to try and obtain a history to establish whether there may be a serious underlying cause such as CNS infection or trauma, and whether there is any history of previous seizures or neurological conditions. Clinical examination should be focused towards signs related to infection–for example, rash or evidence of focal neurological abnormalities, which may suggest more sinister pathology.
In the case of a first seizure, if the seizure is prolonged or recurs within a 24 hour period or if there are abnormal clinical findings, the child should be transferred to hospital for a full assessment. If there is a history of previous febrile seizures and the parents are happy and confident to manage the patient at home they may be discharged. Febrile seizures may recur in around 25%–30% of patients at 2 years therefore it is important that parents are given advice after any episode (Box 4).2
Box 4 Advice to parents following febrile seizures
-
Febrile seizures occur in 2–5% of children aged 6 months to 5 years.
-
They may appear frightening to observers but are generally harmless
-
Simple febrile seizures often occur only once in the first 24 hours of a febrile illness. If the seizure recurs your child should be re-evaluated.
-
A febrile seizure may manifest as body stiffening, twitching of the face or limbs, eye rolling, jerking of the arms or legs, staring or loss of consciousness. They generally last <1 minute but may last up to 15 minutes
-
Your child might appear not to be breathing and the skin colour may become darker. If so, call 999 and lay the child on the floor on his or her back. DO NOT place anything in the child’s mouth.
-
Febrile seizures do not cause brain damage or paralysis
-
Febrile seizures tend to run in families
-
Febrile seizures can recur with subsequent febrile illnesses. Whilst paracetamol or ibuprofen may be used to try and decrease the temperature these have not been shown to prevent febrile seizures.
HEADACHE THE PRIMARY SURVEY POSITIVE PATIENT
A few patients will have obvious serious pathology on ABC evaluation. Any reduction in GCS, acute confusion, focal neurological signs, or petechial rash indicates the need for urgent transfer to hospital. Supportive treatment should be provided as described elsewhere.
Most patients, however, will not have any obvious signs of an immediately life-threatening problem. It is vital that these patients are assessed systematically in order to detect the small proportion of patients with serious pathology. The assessment of a patient with headache can be difficult for the most experienced clinician. Probably the most important factor in headache assessment is the history and time should be spent in specifically eliciting features of the history that may be ‘red flags’ mandating referral to hospital for further investigation and management. Important factors to consider in the history of a headache are summarised in table 3.
Important factors in the history of a headache
 Tip
Tip

Sudden onset headache with maximal severity <15 minutes is a subarachnoid haemorrhage until proven otherwise.
Examination
Examination of a patient with headache should include a complete systems examination as well as a thorough neurological examination. Numerous non-neurological disorders and conditions affecting the eyes, ear, nose, and throat may cause a headache therefore the examination must include assessment of all the following:
Conscious level and mental state examination
Drowsiness or confusion all suggest intracranial pathology or infection. Such patients should be referred to hospital for a full assessment.
Speech
This can easily be assessed whilst taking the history from the patient. Any evidence of slurred speech (dysarthria), or difficulty in word finding (dysphasia) suggests the patient may have had a stroke.
Skull
The skull should be palpated for any areas of tenderness or swelling and inspected for bruising. Tenderness over the temporal area may suggest temporal arteritis and these patients must be referred for an urgent ESR.
Neck pain/stiffness
Neck stiffness may indicate meningeal irritation due to the presence of blood or infection. Ask the patient to put their chin on their chest to see if this increases pain. Kernigs and Brudzinskis sign are useful tests for evidence of meningism.
Eyes
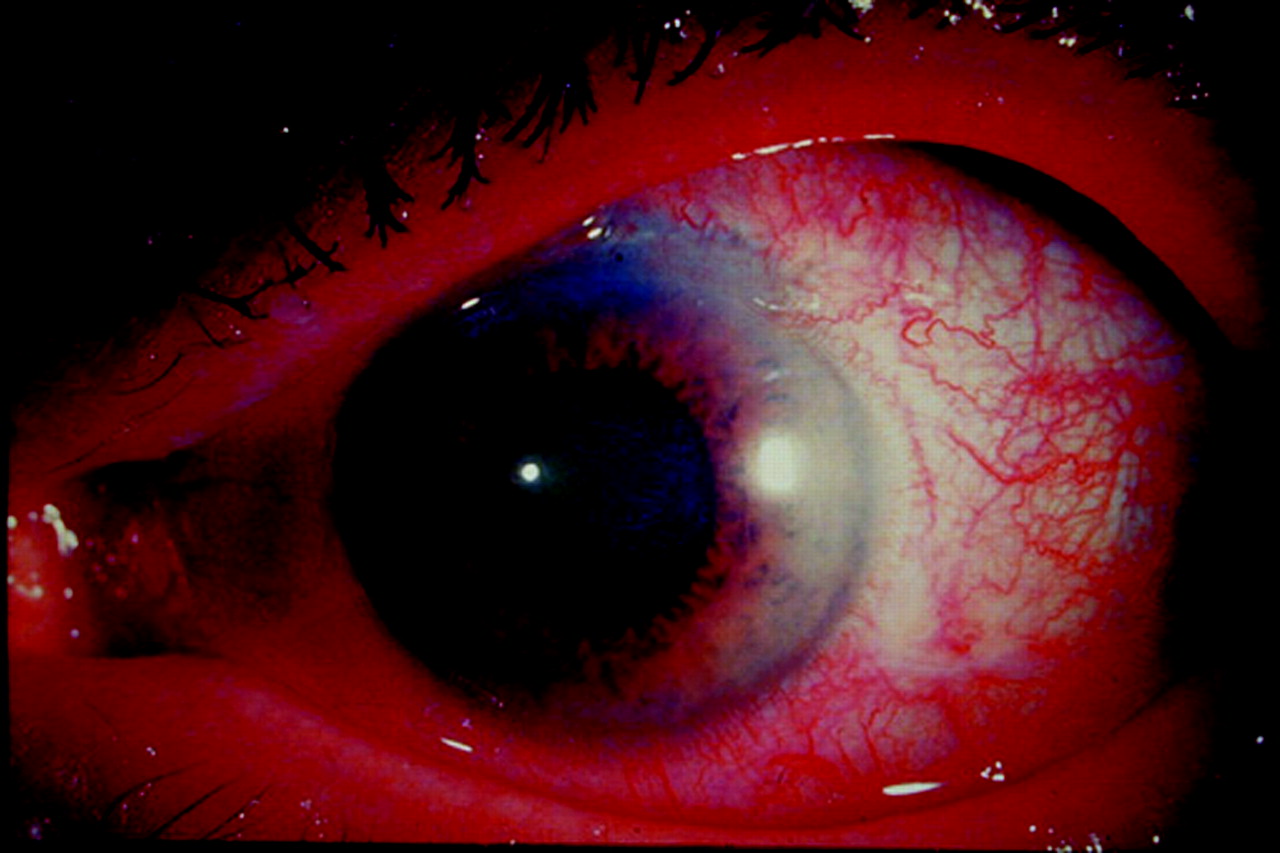
Check pupil reaction at the same time checking for any photophobia. Check for any restriction of eye movement (opthalmoplegia) or diplopia (cranial nerves III, IV, VI) and nystagmus. Check visual acuity and if possible examine the fundi. Rarely serious eye problems such as glaucoma may present with severe headache. There will usually be abnormal eye signs including a red eye, cloudy cornea, irregular mid-dilated pupil and reduced visual acuity (fig 4). If there is any suggestion of glaucoma the patient must be referred immediately for an ophthalmology assessment.

Acute glaucoma.
ENT
Examine the ears and throat for any evidence of infection that may produce headache. Pain on percussion over the sinuses may indicate sinusitis.
General neurological examination
A full neurological examination should be performed as summarised in Box 6.
Box 6 General neurological examination
Signs of meningeal irritation
-
Photophobia
-
Neck stiffness
-
Kernigs sign
Higher mental function
-
GCS
-
Mental state examination
Cranial nerves
-
II – visual acuity and fields
-
III, IV, VI – eye movements
-
V– jaw power and face sensation
-
VII– facial movements
-
VIII–hearing
-
IX–palate movements, swallowing
-
XI– shrugging shoulders
-
XII tongue movement
Limbs
-
Power
-
Tone
-
Reflexes
-
Sensation
-
Co-ordination
-
Balance and gait
Brudzinski’s sign
Passive flexion of the neck induces involuntary hip flexion
Kernig’s sign
With patient supine, flex hip to 90° with knee. When knee is extended, pain is produced in the back of the neck.
Systems examination
Record vital signs, in particular temperature and blood pressure. Malignant hypertension may present with headache and requires urgent treatment in hospital.
Management plan
Following a careful history and examination the practitioner should be able to formulate a differential diagnosis and management plan. All headaches of acute, severe onset require immediate assessment in secondary care in order not to miss subarachnoid haemorrage. Any headache associated with the red flags highlighted in table 3 or abnormal examination findings suggesting a possible serious cause should also be referred. If meningitis is suspected then the patient should be treated with benzylpenicillin or a 3rd generation cephalosporin. This should be given intravenously if possible although the intramuscular route may be used if intravenous access cannot be secured (fig 3).
Headaches of subacute or chronic onset, that are not associated with any red flags or abnormal neurological findings will need further assessment, however, it may be more appropriate to refer these patients to their general practitioner for assessment and outpatient referral if necessary. If patients are discharged they should be advised that if they develop any new features such as vomiting, visual disturbance or other neurological symptoms then they should seek urgent re-assessment. Beware the patient >60 years old with headache of several weeks duration who may not have any abnormal physical findings but who may have temporal arteritis, which untreated may lead to blindness. An urgent blood test for ESR will aid in this diagnosis.
If the history and examination suggest a primary headache syndrome such as migraine then the patient may be treated in the community. However, this diagnosis should only be made without further assessment if the patient has a previous history of migraine that fulfils the diagnostic criteria of the International Headache Society (Box 7).3
Box 7 International Headache Society diagnostic criteria for migraine
-
Lasts 4–72 hours
-
At least 2 of: unilateral location, pulsating quality, moderate to severe intensity, aggravation by routine physical activity
-
At least 1 of: nausea/vomiting, photophobia, phonophobia
-
At least 5 attacks fulfilling the above
-
History and neurological examination do not suggest underlying organic pathology.
Pitfall

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Beware diagnosing migraine if the attack has lasted longer than 72 hours or if there has been incomplete resolution between attacks. Similarly, if the patient says this is the worst episode they have ever had or if it is different from their usual headache pattern they will warrant hospital assessment.
Migraine is best treated by a combination of anti-inflammatory medication (for example, diclofenac) and an anti-emetic (for example, metoclopramide). Alternatively a 5HT agonist such as sumatriptan may be given but remember this is contraindicated in patients >65 years old or if there is a history of ischaemic heart disease or uncontrolled hypertension.
The diagnosis of tension headache may be suggested by a chronic history of bilateral ‘pressing’ or ‘tight’ pain with no systemic disturbance or abnormal neurological symptoms or signs that get worse as the day progresses. It may be associated with a history of depression or medication misuse. Analgesics are unhelpful if the headache is chronic. This diagnosis should not be made until all other causes of headache have been excluded by a thorough medical assessment and appropriate investigations.
Patients complaining of a headache shortly after a head injury may be managed at home if they are fully alert and orientated and have a normal neurological examination. They should be advised to seek medical attention if they have any of the following symptoms:
-
vomiting
-
increased drowsiness or unconsciousness
-
severe or worsening headache
-
double vision
-
severe irritability or major change in behaviour
-
fitting
Any patient who has suffered a significant loss of consciousness or amnesia should be assessed in hospital as they may require a CT brain in accordance with the NICE head injury guidelines.4 A patient complaining of increasing headache days or even weeks after a head injury, particularly if associated with other neurological symptoms or signs may have a subdural haematoma and should be referred for assessment.
SUMMARY
Neurological emergencies are seen relatively common by the community practitioner and require careful assessment in order to identify potential serious pathology. Headache presents a particular diagnostic challenge and a good history and examination is vital to avoid missing potentially life-threatening conditions such as subarachnoid haemorrhage. This article aims to provide a system to guide assessment and management, however, it is clear that in most cases patients will require secondary care assessment. Neurological conditions are extremely frightening for both patients and carers who often fear they may be having a stroke or brain tumour, therefore reassurance and support is a crucial part of the primary care professionals role.
Footnotes
-
Competing interests: none declared