Article Text

Statistics from Altmetric.com
- LVAD
- disconnection
- out-of-hospital
- ventricular assist device
- VAD
- cardiac care
- heart failure
- major incidents
- nursing
- prehospital
- resuscitation
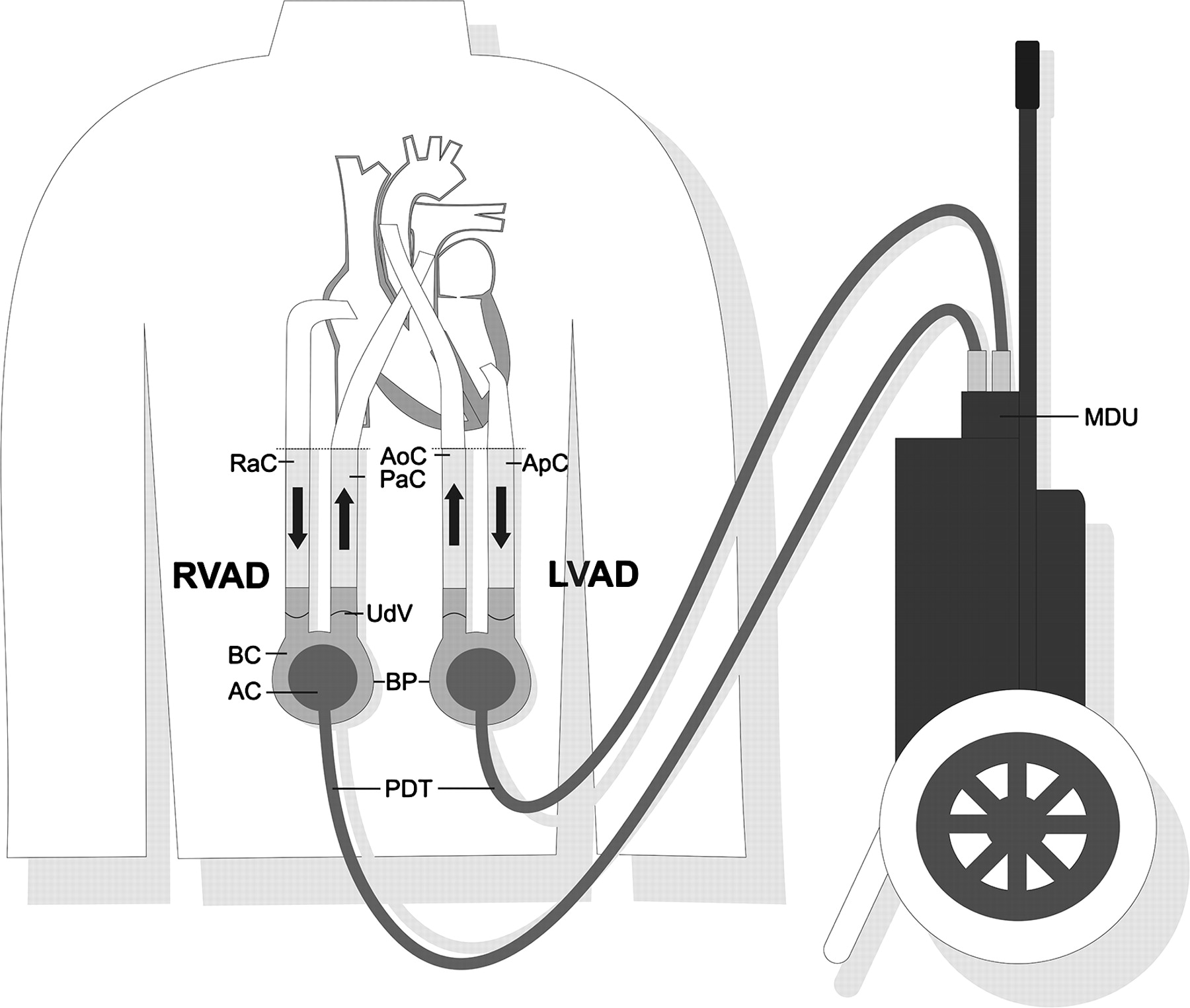
The case of a 63-year-old Caucasian male suffering from secondary dilatative cardiomyopathy due to ischaemic and consecutive valvular heart disease was reported. He had had bypass surgery and mitral valve replacement in 2002 after mitral chord rupture. Five years later, several episodes of arrhythmias occurred (recurrent atrial fibrillation and ventricular tachycardia) and his cardiac function decreased. Echocardiographic examination revealed an ejection fraction of 25% and, subsequently, he was listed for cardiac transplantation. Despite extensive conservative treatment, the patient developed end-stage heart failure and a biventricular ventricular assist device (VAD) (EXCOR VAD ®, Berlin Heart AG, Berlin, Germany, figure 1) was implanted at the end of 2007. The patient recovered from this operation without any complications and was discharged home after receiving specific instruction for VAD management. Regular assessments and controls were performed at the hospital on an outpatient basis.

{kind=link}
Diagram of a biventricular ventricular assist device (VAD) (EXCOR VAD ®, Berlin Heart AG, Berlin, Germany). AC, air chamber; AoC, aortic cannula; ApC, apical cannula (apex of the left heart); BC, blood chamber; BP, blood pumps; LVAD, left ventricular assist device; MDU, mobile driving unit; PaC, pulmonary artery cannula; PDT, pneumatic driving tubes; RaC, right atrial cannula; RVAD, right ventricular assist device; UdV, unidirectional valve.
Five months later, an emergency team based at the Triemli City Hospital responded to an emergency call from the patient's neighbour. During a violent argument between the patient and his 10-year-old son, one of the VAD cannulas (ie, the right atrial cannula, figure 1) was accidentally disconnected. The patient lost consciousness and his son called for help in the neighbourhood. A neighbour re-connected the cannula and started lay cardiopulmonary resuscitation. Upon the arrival of the emergency team 15 min later, pulseless electrical activity was diagnosed and cardiopulmonary resuscitation was resumed according to international guidelines including intubation and mechanical ventilation.
A VAD malfunction was observed and the hospital-based perfusionist on duty was called. He gave instructions by phone on how to re-start the VAD. However, the problem of a potential air-block could not be solved and therefore the manual pump, which is attached to the mobile driving unit of every VAD system, was set in operation. A fire worker at the scene was assigned to pump at a rate of 60–80/min. A sufficient circulation was then established and the patient was transferred to the hospital.
Despite the re-installation of a new VAD pump system and continuous resuscitation efforts, the haemodynamic situation of the patient could not be stabilised during the initial hospital treatment period. Therefore, an extracorporeal membrane oxygenation was successfully initiated. Unfortunately, after establishing adequate haemodynamic support and oxygenation, severe anoxic encephalopathy was diagnosed. All therapeutic measures were discontinued and the patient died 5 h after admission, in the presence of his family.
Heart failure is one of the leading causes of death in the Western world. When conservative drug therapy for end-stage heart failure fails, the only treatment option is heart transplantation.1 Unfortunately, there is a growing imbalance between available organs and recipients. Therefore, the implantation of VAD has become a cornerstone in a ‘bridge-to-transplantation’ concept but, occasionally, is also used as long-term therapy.2 VAD use typically improves the haemodynamic situation of patients suffering from end-stage cardiac disease: End-organ function is better preserved and exercise tolerance increases, allowing patients to be discharged home with a reasonable quality of life.3 Incidence of major adverse events has declined in recent years, and good results in terms of survival, as well as quality of life, for the long-term use of these devices have been reported. However, major complications associated with VAD use are still of concern:2–5 bleeding may occur in up to 40% of VAD patients, thromboembolism and infection was observed in 20% and up to 55% of the cases.
The disconnection of a VAD cannula in a patient managed on an out-of-hospital basis, however, has never been described. The accidental disconnection and major blood loss reported in this case, in combination with the insufficient circulatory support during the time period until the emergency team arrived, may be responsible for the anoxic encephalopathy and consecutive fatal outcome. It emphasises the fact that emergency care teams need to have basic knowledge of VAD pump systems and that they must be prepared to perform basic problem-solving related to these systems. Ideally, information related to VAD patients living at home should be available in order to provide optimal care in an emergency situation. A central registry of these patients and their devices is, therefore, highly desirable, in order to directly distribute information to rescue teams at the scene and to improve communication with hospital-based cardiac surgery specialist teams on duty.
Footnotes
Competing interests None.
Patient consent Obtained from the patient's family.
Provenance and peer review Not commissioned; externally peer reviewed.