Article Text

Abstract
Background The tendency of sepsis to progress rapidly and the benefit of an early start of treatment emphasise the importance of fast risk stratification in the emergency department (ED). The aim of the present work was to validate the Mortality in Emergency Department Sepsis (MEDS) score as a predictor of 28-day mortality in ED patients with sepsis in The Netherlands, and to compare its performance to C reactive protein (CRP) and lactate.
Methods This was a historical cohort study in a secondary and tertiary care university hospital. Patients were included if they were seen by an internist in the ED, fulfilled the clinical criteria for sepsis and were admitted to the hospital. Primary outcome was all-cause in-hospital mortality within 28 days.
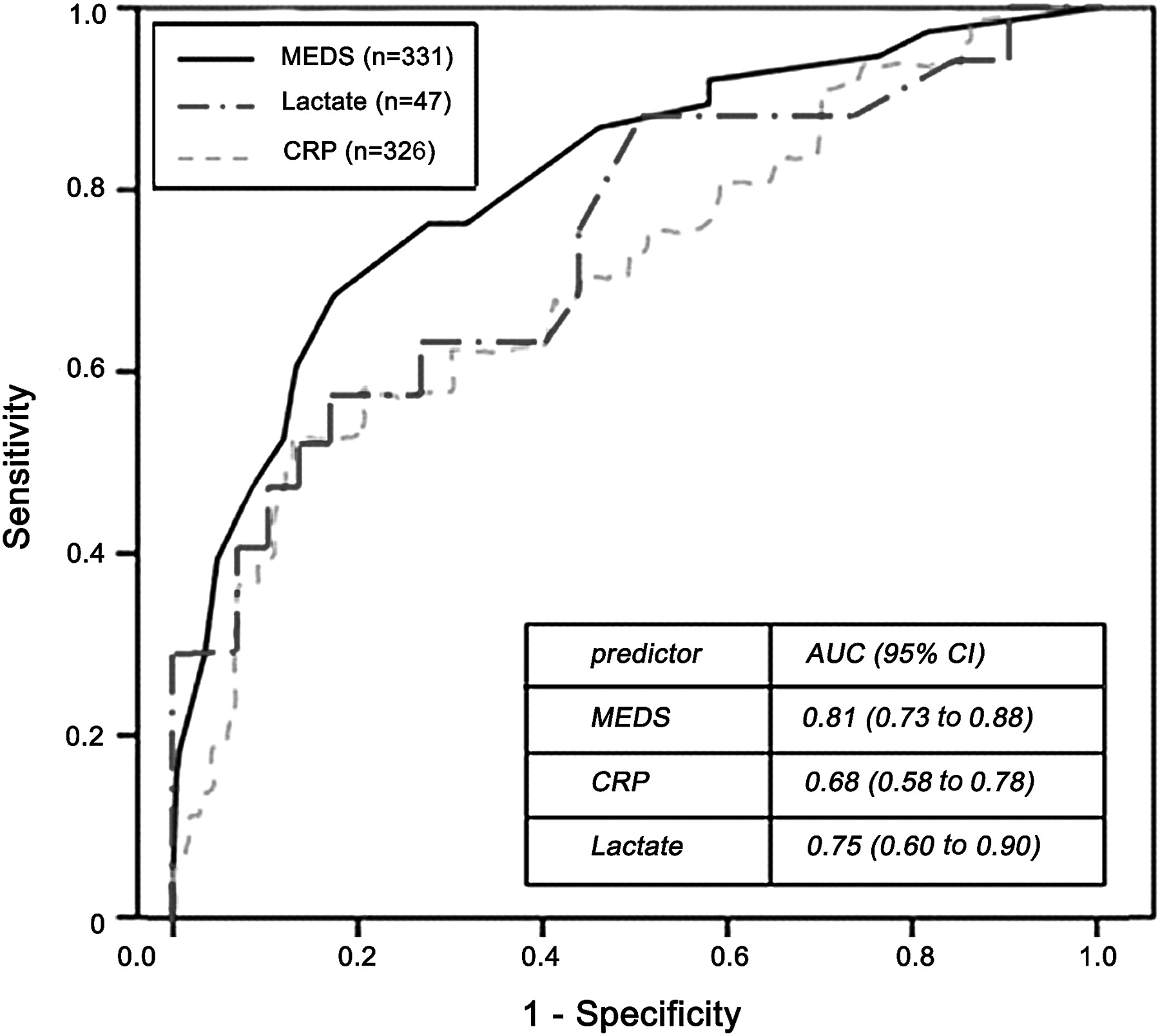
Results In the 6-month study period, 331 patients were included, of whom 38 (11.5%) died. Mortality varied significantly per MEDS category: ≤4 points (very low risk: 3.1%), 5–7 points (low risk: 5.3%), 8–12 points (moderate risk 17.3%), 13–15 points (high risk: 40.0%), >15 points (very high risk: 77.8%). Receiver operating characteristic (ROC) analysis showed that the MEDS score predicted 28-day mortality better than CRP (area under the curve (AUC) values of 0.81 (95% CI 0.73 to 0.88) and 0.68 (95% CI 0.58 to 0.78), respectively). Lactate was not measured in enough patients (47) for a valid evaluation, but seemed to predict mortality at least fairly (AUC 0.75, 95% CI 0.60 to 0.90).
Conclusions The MEDS score is an adequate tool for predicting mortality in patients with sepsis in a Dutch internistic ED population. CRP is less useful in this context. Lactate appears to be at least a fair predictor of mortality, but needs to be investigated more systematically in a larger population.
- Sepsis
- outcome
- mortality
- emergency department
- risk stratification
- mortality in emergency department sepsis score
- C reactive protein
- lactate
- clinical assessment
- education
- assessment
- infectious diseases
- wounds
- infection
Statistics from Altmetric.com
- Sepsis
- outcome
- mortality
- emergency department
- risk stratification
- mortality in emergency department sepsis score
- C reactive protein
- lactate
- clinical assessment
- education
- assessment
- infectious diseases
- wounds
- infection
Introduction
Sepsis is a systemic inflammatory response syndrome (SIRS), provoked by an infection.1 It is a condition with high morbidity and mortality, comparable to that of myocardial infarction or stroke.2 The estimated incidence in The Netherlands is 55:100 000 with in-hospital mortality ranging from 16% in sepsis to 50% in septic shock.3 The incidence has increased in the entire Western world during the last decades, yet mortality has decreased only marginally.4 Despite the high mortality, the severity of sepsis is frequently underestimated.5
Sepsis has a tendency to progress very rapidly to a more severe stage with organ dysfunction. Late recognition and inadequate treatment both contribute to the current high mortality.6 One of the largest improvements in sepsis treatment has been the development of early goal-directed therapy (EGDT), which aims to start treatment within the first 6 ‘golden hours’. The implementation of EGDT has resulted in a relative reduction of 7% to 16% in mortality in some hospitals.7 A reliable risk stratification tool could improve the management of sepsis by increasing awareness of the seriousness of the condition, assisting in the best choice of treatment and by accelerating transfer from the emergency department (ED) to the intensive care unit (ICU) or general ward through more effective communication between professionals. Furthermore, the tool may be used for research purposes.
Several laboratory tests are used to assess the severity of sepsis, such as C reactive protein (CRP) and lactate tests. CRP is widely used, and has turned out to be a weak prognostic tool in other research.8 Arterial lactate is frequently used as a marker of hypoperfusion, which is often present in severe sepsis and septic shock. The value of lactate assessment in the ED for predicting the outcome of sepsis has been investigated previously, but mainly in patients with severe sepsis and septic shock. Lactate was a moderate predictor of mortality with area under the curve (AUC) values ranging from 0.62 to 0.87.9–11
There was no compound scoring system to reliably predict the risk of mortality in ED patients with sepsis until Shapiro et al12 published the Mortality in Emergency Department Sepsis (MEDS) score in 2003. Scores that were developed earlier, such as the Acute Physiology and Chronic Health Evaluation II (APACHE II), are not feasible for an ED setting because they include parameters not commonly obtainable to the ED doctor.13 In contrast, the MEDS score is a simple scoring system containing parameters that are readily available. In several studies, the MEDS score adequately predicted mortality in ED patients who were suspected of having sepsis.12 14–19
An ED patient in The Netherlands may differ from patients in the USA because of differences in the way the healthcare system is organised. In The Netherlands, primary healthcare has a so-called gatekeeper function: patients cannot visit an ED without first consulting a general practitioner, in contrast to the USA. Because of this difference in organisation of the healthcare system, the MEDS score, which was developed in the USA, had to be validated in a Dutch ED population before implementing it into daily practice.
Our main objective was to validate the MEDS score as a predictor of 28-day mortality in patients with sepsis, severe sepsis or septic shock who present to the ED of a university hospital in The Netherlands. The second objective was to compare the performance of the MEDS to that of serum CRP and arterial lactate levels.
Materials and methods
Study design and setting
After obtaining approval of the Medical Ethics Committee, we performed a historical cohort study in a secondary and tertiary care university hospital in The Netherlands. Maastricht University Medical Centre (MUMC) has 715 beds and an ICU capacity of 21 beds. Annually, an average of 22 750 patients visits the ED, of whom 5075 are specifically referred by the general practitioner to the internist. In The Netherlands, patients cannot visit an ED without being referred by a general practitioner, except for high emergency (ambulance) patients and a few self-presenters. In the ED, an acute internist assesses these (mostly) referred patients and decides on further treatment, including admittance to the hospital and consulting an intensivist. There are emergency doctors in our ED.
Selection of participants
By reviewing the ED charts of everyone who attended the ED between 1 August 2009 and 1 February 2010, we included every patient who was over 18 years of age, who was examined by an internist, who fulfilled the clinical criteria for sepsis, severe sepsis or septic shock according to the Society of Critical Care Medicine (SCCM) International Sepsis Definitions Conference 2001,1 and was admitted to the hospital.
Because the MEDS score was originally developed in a group of patients selected based on the criterion of having blood cultures taken in the ED,12 we also selected all patients seen by an internist, whose blood was cultured regardless of the above-mentioned sepsis criteria.
Outcome measures
The primary end point was all-cause in-hospital mortality within 28 days of ED presentation, as recorded in the hospital's electronic database. Patients who were discharged alive within 28 days were regarded as survivors, presuming the decision of discharge as the end of the critical period, according to the definition used by Shapiro et al.12
Clinical sepsis severity categories
These were as follows:
SIRS. Presence of two or more of the following criteria: (1) heart rate >90 beats/min, (2) body temperature >38°C or <36°C, (3) respiratory rate of >20 breaths/min or PaCO2 of <4.3 kPa, (4) white blood cell count >12×104 cells/ml or <4×104 cells/ml.1
Sepsis. SIRS with an infection as the most likely cause. Possible signs of infection included: urinary tract symptoms, coughing or dyspnoea, mental status changes, hypotension, fever or chills, skin or joint symptoms, gastrointestinal symptoms, signs of meningeal irritation, or elevated plasma CRP.
Severe sepsis. Sepsis with signs of acute organ dysfunction or hypoperfusion, namely: an acute rise in serum creatinine, acute oliguria; an acute rise in serum transaminases, bilirubin >30 mmol/litre; any change in baseline mental status/GCS<15; platelets <100×109 cells/litre or other signs of acute coagulopathy; oxygen saturation <90%, respiratory rate >20 breaths/min, or need for mechanical ventilation; hyperglycaemia without a history of diabetes; acute elevation of cardiac enzymes, systolic blood pressure <90 mm Hg, capillary refill >2 s, mottled skin, or metabolic acidosis.
Septic shock. Severe sepsis in the presence of hypotension (systolic blood pressure <90 mm Hg) refractory to adequate fluid resuscitation20 and/or an arterial lactate level ≥4 mmol/litre.
Using these categories does not exclude a certain level of uncertainty, particularly in an ED setting, because an infection cannot fully be proven as the cause of the symptoms in that early phase. It would therefore be more correct to speak of suspected or clinical sepsis. For the remainder of this paper, we will use the term sepsis to refer to the broader entity of suspected or clinical sepsis.
MEDS score
Definitions and criteria for determining the MEDS score were adopted from Shapiro et al.12 Terminal illness was defined as a chance of >50% of dying in the next 30 days and/or the presence of metastatic cancer. Respiratory difficulty was defined as an oxygen saturation <90%, respiratory rate >20 breaths per minute or an arterial pCO2 of <4.3 kPa. Septic shock was defined according to the criteria described above. Lower respiratory tract infection was defined as a suspected or proven infection, for example by an infiltrate on chest x-ray. Finally, altered mental status was defined as any difference from the patient's baseline in orientation or alertness. The total score was divided into five categories, as shown in tables 1 and 2.
Mortality in Emergency Department Sepsis (MEDS) score
Mortality in Emergency Department Sepsis (MEDS) category and mortality percentages
Data collection and processing
All data were retrospectively retrieved from the ED charts and the electronic database of the hospital. We recorded date of visit, demographic data, vital parameters, severity of sepsis, diagnosis and focus of infection, comorbidity, laboratory results, items of the MEDS score, moment of antibiotic administration and door-to-needle time (time between arrival at the ED and administration of antibiotics) and unit of admittance (general ward, medium care unit (MCU) or ICU). As we assessed the value of the MEDS score in the ED, the diagnosis ‘sepsis’ and the severity of sepsis made by the treating doctor at the moment the patient left the ED was chosen as the main diagnosis (working diagnosis) and not the diagnosis made at the moment of hospital discharge.
Data analysis
All statistical analyses were performed with SPSS V.16.0 (SPSS, Chicago, Illinois, USA). Categorical data were reported as absolute counts with percentages, continuous data were reported as mean (SD). Tests for association were carried out if possible and relevant using Fisher's exact test, Mann–Whitney U test or analysis of variance (ANOVA). ANOVA was also used for the test for trend of death rates over the MEDS categories. Associations were considered statistically significant if p<0.05. Receiver operating characteristic (ROC) curves were constructed and the AUC with 95% CI was calculated as a measure of discriminative ability on 28-day mortality. An AUC of 1.0 represents perfect, and an AUC of 0.5 no discriminatory ability.
Results
In our 6-month study period, 2498 ED patients were seen by an internist, of whom 858 patients were admitted to the hospital. In all, 338 (39.4%) of these were suspected of having sepsis at the moment of their ED presentation and were therefore included in our study. We excluded 7 patients because of missing essential data (vital parameters and/or MEDS items), to form a final database of 331 patients.
Table 3 summarises characteristics of the study population. In all, 38 patients died (11.5%). Of the clinical severity categories, sepsis was most prevalent (66%), followed by severe sepsis (30%) and septic shock (4%).
Patient characteristics and management
MEDS score
Mortality increased per subsequent MEDS category (figure 1). The mortality was 3.1% in the category ≤4 points, 5.3% for 5–7 points, 17.3% for 8–12 points, 40.0% for 13–15 points and 77.8% for the category of >15 points (test for trend: p<0.001). Figure 2 shows the ROC curve for the discriminative ability of the MEDS score with an AUC of 0.81 (95% CI 0.73 to 0.88).

Mortality per Mortality in Emergency Department Sepsis (MEDS) category (%).

{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curves for Mortality in Emergency Department Sepsis (MEDS), C reactive protein, and lactate.
The characteristics of patients and offered treatment per MEDS category are shown in table 4 The MEDS score was generally, but not consistently, higher in the patients with more severe forms of sepsis. The mean CRP and lactate levels were somewhat higher with increasing MEDS scores, but CRP and lactate levels did not rise consistently with increasing MEDS scores. Some patients did not receive standard treatment if they had an advanced care directive, a palliative treatment was preferred or restrictions were agreed on grounds of medical futility. Comparing our patients to the original validation set of Shapiro et al12 (table 5), we found higher death rates, especially for the high-risk and very high-risk groups (40.0 vs 16.1% and 77.8 vs 39.0%, respectively). However, the distribution of the MEDS score categories was quite similar in the two populations, with increasing mortality for increasing MEDS scores. In our population, there were more patients with malignancy and terminal illness, and fewer patients with congestive heart failure and HIV than in the population of Shapiro et al.
Characteristics and management per Mortality in Emergency Department Sepsis (MEDS) category
Study population versus the original validation set
The group of patients whose blood was cultured, irrespective of the sepsis diagnosis, consisted of 372 people. This group did not differ from our primary study group with sepsis regarding demographic characteristics (data not shown). Roughly 25% of these blood culture patients did not fulfil the criteria for SIRS, while 50% had sepsis, 22% severe sepsis and 3% septic shock. The overall mortality was 8.6%, while the mortality per MEDS category was similar to the death rates of the study group with sepsis. The AUC of the MEDS score was 0.85 (95% CI 0.77 to 0.92) for this culture group.
CRP and lactate levels
CRP levels were measured in 326 patients of the primary sepsis group, of whom 38 died (11.7%). Death rates of patients with CRP levels <100 and ≥100 mg/litre were 7.6% (SD 2.2) versus 14.9% (SD 2.6), respectively (p=0.038). The AUC of CRP was 0.68 (95% CI 0.58 to 0.78; figure 2).
Arterial lactate levels were measured in 47 patients of the primary sepsis group, of whom 17 died (36.2%). Death rates of patients with lactate levels ≤4 and >4 mmol/litre were 24.2% (SD 7.5) versus 74.3% (SD 12.8), respectively (p=0.001). The AUC of lactate was 0.75 (95% CI 0.60 to 0.90; figure 2). Of the patients in whom lactate was measured, 21% had sepsis, 51% had severe sepsis and 28% had septic shock at ED presentation.
Discussion
In this study, we investigated the value of the MEDS score in predicting mortality of sepsis at the Emergency Department. We found an AUC of 0.81 and significantly different death rates per MEDS category, which confirms the MEDS score as a good risk stratification tool in ED patients with sepsis who are treated by an internist. These results are comparable to those of the original validation study and to other studies, which found AUCs ranging from 0.74 to 0.88.15–19 22 The mortality in our population was higher than in the original validation set of Shapiro et al,12 especially in the high-risk and very high-risk groups (40.0 vs 16.1% and 77.8 vs 39.0%, respectively). A possible explanation for the higher mortality in our study is the higher prevalence of terminal illness and malignancy in our patients. A second explanation may be the different healthcare organisation in The Netherlands, which may result in an ED population that is more seriously ill because of the preselection by the primary healthcare.
To optimally compare our results to those of the original validation study, we also created a group of patients based on the same inclusion criteria as Shapiro et al,12 namely the patients, whose blood was cultured, regardless of clinical signs of sepsis. The overall mortality of these 372 patients was 8.6%, compared to 11.5% in our primary study population with sepsis. This difference can be explained by the fact that 25% of the patients in the ‘blood culture group’ did not fulfil the criteria for SIRS and were probably less severely ill. ROC analysis showed a slightly higher AUC (0.85) than in our primary study population with sepsis. We believe that the inclusion criteria that we used are more adequate in defining sepsis than the criterion of ordering blood cultures, and we thus validated the MEDS in patients for whom the score was actually developed: those in whom sepsis is suspected at ED presentation.
The MEDS score is a good predictor of mortality and is particularly feasible in the ED setting, as all items are readily available. Furthermore, the inter-rater reliability of the MEDS is high, meaning that the score as a whole was reproducible (κ 0.93 as found by Sankoff et al19). A possible improvement of the MEDS score might be the combination with lactate. This may not be difficult to implement in clinical practice because it was shown that venous lactate levels are similar to arterial levels and, therefore, obtaining an arterial lactate sample is not necessary.23
Obviously, the most important practical consequence of the implementation of the MEDS score is the impact on therapeutic decisions. The MEDS score can be used to increase the awareness of doctors on the high death rates of sepsis. Thereby patients would hopefully receive more timely and appropriate treatment, which is expected to reduce morbidity and mortality as already has been shown in hospitals that have implemented EGDT.7 Furthermore, improvement of treatment is likely to result in lower sepsis-related costs and a shorter duration of in-hospital stay. One should realise that the MEDS score only estimates the chance of dying. It does not directly indicate how to treat patients and is therefore not immediately usable as a decision tool, nor does it provide a treatment protocol. The impact of clinical use of the MEDS score on therapeutic decision making has not been studied yet.
As well as validating the MEDS score, we investigated the discriminative ability of CRP and lactate and compared these to that of the MEDS score. Like in other studies,16 17 19 the MEDS was the best predictor of mortality. The discriminative ability of CRP for 28-day mortality was poor (AUC: 0.68). Other studies have found similar results for the value of CRP in predicting mortality in ED sepsis.21 24 Lactate seemed a fair predictor of mortality (AUC: 0.75), which is similar to other studies reporting AUCs ranging from 0.62 to 0.87.9–11 However, we did not measure lactate in enough patients to provide a precise estimate. This finding suggests that our doctors, like others,5 tend to underestimate the gravity of the disease in patients with sepsis, as a lactate should be measured in all patients with severe sepsis and septic shock. Furthermore, our results may be an underestimate, since most measured values were from severely ill patients.
Limitations
Our study has some limitations. First, we depended on the notes of the attending doctor for obtaining all the necessary information, which could have led to information bias because some relevant information may not have been properly recorded and we had to exclude seven patients due to missing data. In addition, the judgement about life expectancy (needed to score the item of terminal illness) was made retrospectively by the authors based on the patient records. Moreover, the use of 28 day in-hospital mortality as the end point is arbitrary for two reasons. First, mortality was recorded in a group of patients who did not receive standardised treatment. The death rate was therefore dependent on the severity of the disease at the moment of presentation in the ED and on decisions about treatment. Therefore, our results cannot be directly used to guide treatment decisions. Second, the influence of sepsis on mortality may extend further than the first 28 days after the start of illness.
Conclusions
The MEDS score appeared to be a good predictor of 28-day mortality in a Dutch secondary and tertiary care university hospital. The MEDS is able to stratify ED patients with sepsis, who are treated by an internist, into groups with clinically significant differences in death rates, as it has an AUC of 0.81. The death rates in our population were higher than in the original validation set from the USA, especially in the high-risk and very high-risk groups. CRP was less useful as a predictor of mortality (AUC: 0.68). Lactate seemed to be at least a fair predictor (AUC: 0.75), but needs to be investigated more systematically in a larger population.
References
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the Medical Ethical Committee Maastricht University Center.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Primary survey