Article Text

Abstract
Background Traumatic brain injury is a common ED presentation. CT-head utilisation is escalating, exacerbating resource pressure in the ED. The biomarker S100B could assist clinicians with CT-head decisions by excluding intracranial pathology. Diagnostic performance of S100B was assessed in patients meeting National Institute of Health and Clinical Excellence Head Injury Guideline (NICE HIG) criteria for CT-head within 6 and 24 hours of injury.
Methods This multicentre prospective observational study included adult patients presenting to the ED with head injuries between May 2020 and June 2021. Informed consent was obtained from patients meeting NICE HIG CT-head criteria. A venous blood sample was collected and serum was tested for S100B using a Cobas Elecsys-S100 module; >0.1 µg/mL was the threshold used to indicate a positive test. Intracranial pathology reported on CT-head scan by the duty radiologist was used as the reference standard to review diagnostic performance.
Results This study included 265 patients of whom 35 (13.2%) had positive CT-head findings. Within 6 hours of injury, sensitivity of S100B was 93.8% (95% CI 69.8% to 99.8%) and specificity was 30.8% (22.6% to 40.0%). Negative predictive value (NPV) was 97.3% (95% CI 84.2% to 99.6%) and area under the curve (AUC) was 0.73 (95% CI 0.61 to 0.85; p=0.003). Within 24 hours of injury, sensitivity was 82.9% (95% CI 66.4% to 93.44%) and specificity was 43.0% (95% CI 36.6% to 49.7%). NPV was 94.29% (95% CI 88.7% to 97.2%) and AUC was 0.65 (95% CI 0.56 to 0.74; p=0.046). Theoretically, use of S100B as a rule-out test would have reduced CT-head scans by 27.1% (95% CI 18.9% to 36.8%) within 6 hours and 37.4% (95% CI 32.0% to 47.2%) within 24 hours. The risk of missing a significant injury with this approach would have been 0.75% (95% CI 0.0% to 2.2%) within 6 hours and 2.3% (95% CI 0.5% to 4.1%) within 24 hours.
Conclusion Within 6 hours of injury, S100B performed well as a diagnostic test to exclude significant intracranial pathology in low-risk patients presenting with head injury. In theory, if used in addition to NICE HIGs, CT-head rates could reduce by one-quarter with a potential miss rate of <1%.
- Computed tomography
- Diagnostic Tests
- management
- craniocerebral trauma
Data availability statement
Data are available upon reasonable request. All data supporting the findings in this study are available from the author on reasonable request.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
S100B has shown promise diagnostically as an objective marker to rule out intracranial injuries in patients presenting to the ED with head injury. However, evidence assessing the the value biomarkers add to existing clinical guidelines in low-risk patients is limited.
WHAT THIS STUDY ADDS
This study demonstrates that in low-risk adult patients presenting to the ED within 6 hours of head injury, who meet National Institute of Health and Clinical Excellence Head Injury Guideline (NICE HIG) criteria for CT-head, S100B has a negative predictive value of 97%. Theoretically, CT-head requests could reduce by 27%, and 24% of patients could be discharged from the ED without waiting for a CT-head scan. Although the negative predictive value of S100B measured within 24 hours of head-injury remains high at 94%, the risk of missed injury increases from 0.75% to 2%.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Within 6 hours of head injury, S100B has the potential to reduce CT-head demand in adult patients presenting to the ED, with a very low rate of missed injury. This could potentially benefit EDs by reducing overcrowding, resource burden and healthcare costs; and from the patients’ perspective, enable shorter waits, earlier intervention and earlier discharge. Further research should focus on optimising the performance of S100B in addition to the NICE HIG in low-risk patients presenting to the ED within 6 hours of head injury.
Background
Traumatic brain injury (TBI) is a global public health issue responsible for significant morbidity and mortality.1 TBI care requires thorough clinician history and neurological examination in order to identify patients at risk of significant intracranial injury who may need a CT-head scan.2 Increased accessibility has enabled exponential increases in CT-head scan requests from the ED3; however, the diagnostic yield has not increased proportionally.3 In fact, 90% of CT-head scans requested for TBI are normal.4 5 Increasing CT-head scan requests from EDs combined with expanding resource pressure and ED crowding6 ultimately mean that patients are waiting longer to be assessed and waiting longer for CT-head scans.7 It is postulated that the use of objective clinical biomarkers, such as S100B, could better risk stratify patients and better target resources in patients with TBI.8
S100B is a neurotrophic calcium-binding protein that is most abundant in glial cells in the brain and central nervous system. It is also present in adipose tissue, cardiac and skeletal muscles.9 S100B release from glial cells increases in response to injury, and where it normally has a neuroprotective effect, in excess, it can exacerbate neuroinflammation and neuronal dysfunction.10 S100B can be detected in peripheral blood samples following head trauma; but as it is also present in other tissues, S100B levels can also rise in the presence of extracranial trauma.11 Despite this, S100B has been shown to be a sensitive marker for detecting intracranial pathology on CT-head scans and could potentially be used as a screening test to safely reduce CT-head scans in ED.12 13
The optimal time to measure S100B has not been identified, as it has a short half-life (30–90 min).14 The Scandinavian Neurotrauma guidelines,15 incorporating S100B testing into CT-head decision rules, advise on testing S100B within 6 hours of head injury. This approach has been prospectively validated,16 but the prospective study also reported that the guideline could potentially be used within 24 hours of head injury.16 There are limited data regarding the safety and economic benefits of S100B should it be introduced in wider ED settings with different clinical care models.17 Evidence demonstrating that S100B adds value to existing clinical guidelines beyond the Scandinavian model is sparse, particularly the National Institute of Health and Clinical Excellence Head Injury Guidelines (NICE HIGs)18 that are commonly used in Australasian and UK EDs.17 There is also little evidence reviewing the diagnostic performance of S100B in low-risk patient cohorts where S100B is most likely to add clinical and economic value.
Therefore, this study assessed the diagnostic performance of S100B in an Australasian ED setting that uses the NICE HIG for CT-head decision-making in patients presenting to the ED with low-risk head injuries.
Aim
To investigate if S100B can safely rule out significant intracranial injuries in adult patients who present to the ED within 6 and 24 hours of head injury.
Methodology
Study design and setting
This is a prospective observational study conducted across two study sites: Wellington Regional Hospital ED (WRHED) and Hutt Hospital ED (HHED). The Standards for Reporting of Diagnostic Accuracy Studies (STARD) checklist was adhered to when designing and reporting this study.
WRHED is a tertiary referral centre and has an annual census of 75 000 patients. HHED is a regional centre and sees 50 000 patients annually. Both hospitals are publicly funded and work to mandatory 6-hour targets for ED length of stay (LOS).19 The NICE HIGs are used as a clinical decision tool at both sites.4 18 CT scans are available 24 hours a day.
Recruitment and eligibility
Convenience sampling methods were used to identify and screen patients for eligibility between 18 May 2020 and 19 June 2021. Investigators screened patients according to their own availability. Most investigators were clinical ED staff who attempted to recruit patients during their shifts enabling regular out-of-hours recruitment. Others were research students who tended to recruit during standard office hours.
Inclusion criteria: ability to give informed consent, competent, GCS 15, no ongoing post-traumatic amnesia (PTA), ≥18 years of age, presenting within 24 hours of head injury and non-contrast CT-head performed to exclude acute intracranial injury.
Exclusion criteria: pre-existing acute brain injury at time of presentation, such as previous TBI or recent stroke (within 4 weeks); pre-existing neurological condition such as moderate to severe dementia, acute psychosis, multiple sclerosis or motor neuron disease.
CT-head scanning
Patients were assessed by ED doctors in line with current clinical practice. If a CT-head was deemed appropriate, patients were screened for eligibility and informed written consent was obtained.
A significant intracranial injury on CT scan was defined as the presence of any of the following criteria:20 skull fracture, pneumocephalus, intracranial haemorrhage or contusion, diffuse axonal injury, signs of herniation or any other acute traumatic intracranial pathology. Patients with CT scans meeting these criteria were recorded as CT-positive, and those not meeting these criteria were recorded as CT-negative.
Blood sampling
A venous blood sample was drawn at the time of study enrolment into an serum seperating tube (SST) tube and stored in a fridge below 4°C. Blood samples were centrifuged at 3000 rpm for 10 min according to investigator availability within 72 hours.21 22 Serum was pipetted into aliquots and frozen at −80°C. S100B was batch tested using a Cobas Elecsys-S100 module (Roche Diagnostics, NZ, Auckland, New Zealand) in the SCL laboratory in Wellington Regional Hospital. The Cobas Elecsys-S100 module uses an electro-chemiluminescence immunoassay for the in vitro quantitative determination of S100B serum. The lower limit of detection is <0.005 µg/L. The reference standard for S100B to rule out S100B has been clinically validated at 0.1 µg/mL.12 13 Patients with S100B >0.1 µg/mL were recorded as a positive test and those <0.1 µg/mL recorded as a negative test.
Data collection
Data were collected for baseline demographics, anticoagulant use, mechanism, time of injury, presenting features, CT-head results, neurosurgical requirements, admission status and S100B levels. CT-head reading was performed by the on-call duty radiologist and was obtained from the clinical reporting systems.
Primary outcome
To determine the diagnostic accuracy (sensitivity, specificity and negative predictive value (NPV)) of S100B drawn within 6 hours in patients presenting with head injury meeting NICE HIG criteria for CT-head, using acute pathology on CT-head (positive vs negative CT) as the reference standard.
Secondary outcome
To determine the diagnostic accuracy (sensitivity, specificity & NPV) of S100B drawn within 24 hours in patients presenting with head injury who meet NICE HIG criteria for CT-head.
Statistical methods and data analysis
Demographic and clinical features as well as the diagnostic ability of S100B to rule out intracranial injury were described statistically using SPSS software, V.26.0 (IBM Corp). To describe the data, frequency and proportions with 95% CIs and medians with IQRs were calculated as appropriate. To review diagnostic performance, receiver operator curve analysis was conducted as well as sensitivity, specificity, NPV and positive predictive value (PPV) calculations using standard 2×2 box plots. Data outputs are divided into comparator groups for patients who had S100B measured within 24 hours and 6 hours of head injury. χ2 tests or Fisher’s exact tests were used to compare proportions and Mann-Whitney U testing was performed to compare continuous skewed data. The null hypothesis was that there would be no difference between the 6-hour and 24-hour groups. Patients were only included in analysis if S100B biomarker and CT-head results were available. Missing data from other variables were not included in statistical testing.
Sample size
This was estimated based on the CIs that we would see around NPV and PPV. Our aim was to have 95% CIs of <±5%.
Results
Case selection, baseline demographics and presenting features
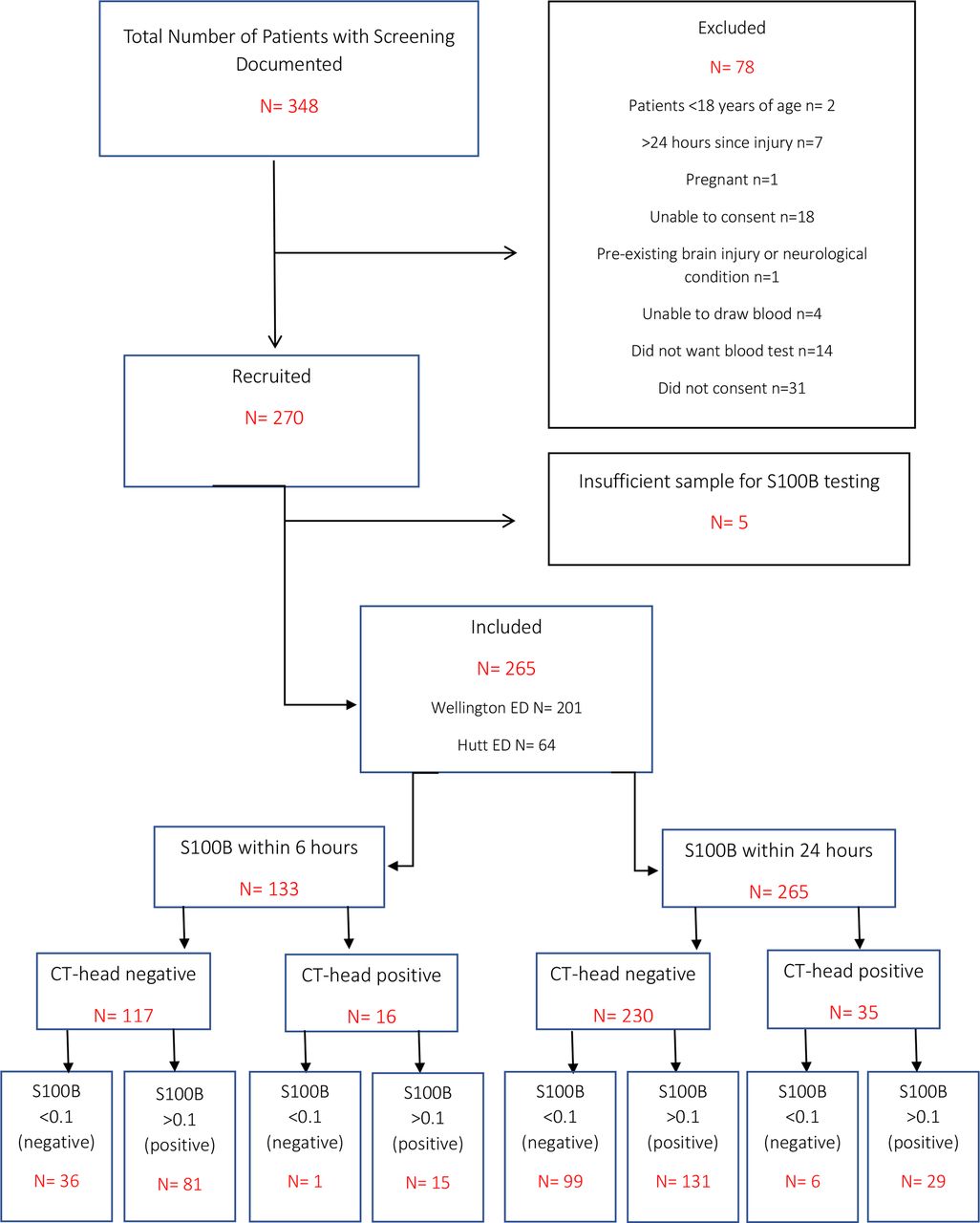
There were 265 included patients (figure 1). There were no significant differences in baseline demographics or clinical presenting features between 6-hour and 24-hour groups (table 1).
Demographics and presenting features

Case selection process and flow of participants through study.
CT-head indication, CT-head timing, CT-head results and patient outcomes
Detailed results are reported in table 2. The most common indication for CT-head according to NICE HIG was current anticoagulation treatment (66 of 251 (26.3%)). Those in the 6-hour group were more likely to have dangerous mechanism as the CT-head indication compared with the 24-hour group (29.% vs 18.5%; p=0.04). The 6-hour group had shorter wait times to CT between the injury and CT-head scan performance (6-hour group: 3.8 (IQR 2.5–5.2) hours vs 24-hour group: 5.2 (IQR 3.5–7.5) hours; p<0.01). There were no wait time differences between groups once patients had presented to the ED.
CT-head indication, results and patient outcomes
There were 16 of 133 (12%) and 35 of 265 (13.2%) positive CT-head scans in the 6-hour and 24-hour groups, respectively. Most common findings were subdural haematoma (14 of 35; 40%), subarachnoid haemorrhage (13 of 35; 37.1%) and other intracranial haemorrhages (11 of 35; 31.4%). Five cases (14.3%) had a base of skull fracture and 10 of 35 (28.5%) had another skull fracture. No patients had an extradural bleed. There were no significant differences between the 6-hour and 24-hour groups with regard to type of traumatic pathology. No patients required acute neurosurgical intervention, but 11 (8.3%) were admitted to hospital for neurosurgical monitoring.
There were 76 of 133 (57.1%) and 132/265 (49.8%) patients discharged from the ED in the 6-hour and 24-hour groups, respectively. Median ED LOS was 5.3 (IQR 3.5–7.0) hours in the 6-hour group with 65.0% (95% CI 47.3% to 82.7%) meeting the 6-hour LOS target. Median ED LOS was 6.0 (IQR 4.2–7.9) hours in the 24-hour group with 49.7% (95% CI 39.3% to 60.1%) meeting the 6-hour LOS target.
Diagnostic performance of S100B
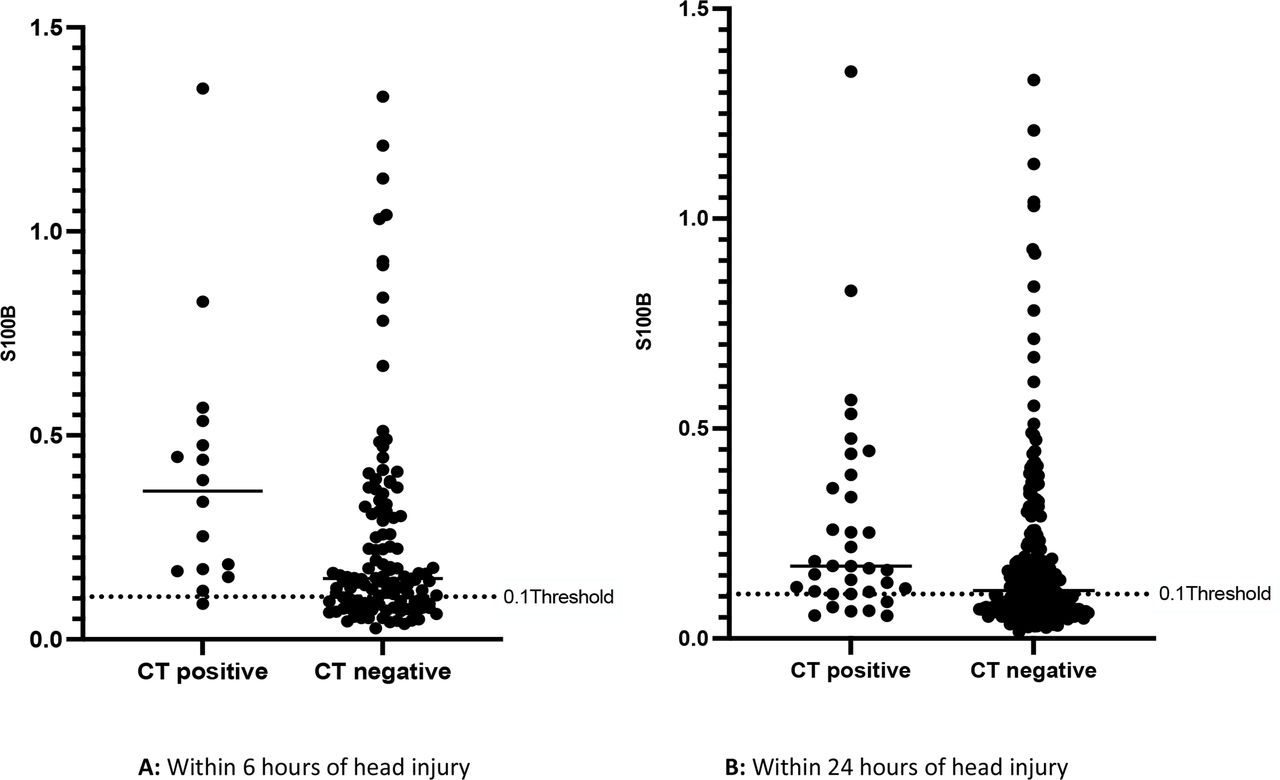
Diagnostic performance of S100B is presented in table 3 and figures 2 and 3. Within the 6-hour group, median S100B for those with positive scans was 0.36 (IQR 0.17–0.52) compared with 0.15 (IQR 0.09–0.31) for those with negative scans (p<0.01). In the 24-hour group, median S100B for those with positive CT-head scans was 0.17 (IQR 0.11–0.39) compared with 0.11 (IQR 0.07–0.22) in those with negative scans (p=0.04). The median S100B levels observed in those with positive CT-head scans were substantially higher in the 6-hour compared with the 24-hour group (p<0.001).
Diagnostic performance of S100B
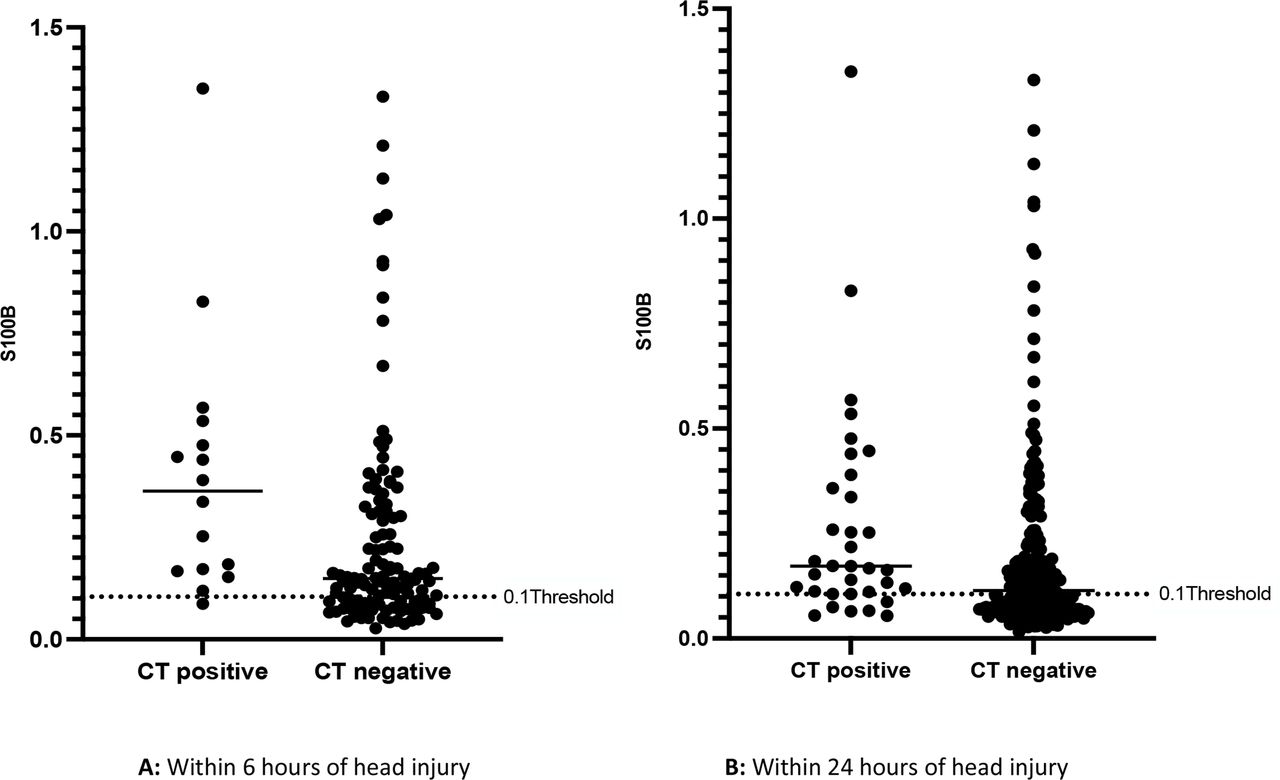
Graphical display of individual S100B results according to CT result: (A) within 6 hours of head injury and (B) within 24 hours of head injury.

{kind=link}
{kind=link}
{kind=link}
Receiver operator curve analysis of S100B within (A) 6 hours and (B) 24 hours of injury. AUC, area under the curve.
The sensitivity of S100B in the 6-hour group was 93.8% (95% CI 69.8% to 99.8%%) and specificity was 30.8% (22.6% to 40.0%). The NPV was 97.3% (95% CI 84.2% to 99.6%). The area under the curve (AUC) was 0.73 (95% CI 0.61 to 0.85; p=0.003). The sensitivity of S100B at 24 hours was 82.9% (95% CI 66.4% to 93.44%) and specificity was 43.0% (95% CI 36.6% to 49.7%). The NPV was 94.29% (95% CI 88.7% to 97.2%). The AUC was 0.65 (95% CI 0.56 to 0.74; p=0.046).
If the clinically validated threshold of 0.1 µg/mL cut-off threshold for S100B had been used to determine CT-head use, and the 37 patients with S100B below this threshold did not proceed to CT, CT-head use would have been reduced by 27.1% (95% CI 18.9% to 36.8%) in the 6-hour group. At 24 hours, 105 patients had S100B values below 0.1 µg/mL equating to a theoretical reduction of 37.4% (95% CI 32.0% to 47.2%) of CT-head requests. One (0.75% (95% CI 0.0% to 2.2%)) patient with an acute traumatic CT-head finding would have been missed within 6 hours, and six (2.3% (95% CI 0.5% to 4.1%)) would have been missed within 24 hours.
When reviewing the subset of patients who were discharged from the ED following a negative CT-head scan, 18 of 76 (23.6%, 95% CI 12.7% to 34.6%) in the 6-hour group and 47 of 132 (35.6%, 95% CI 25.4% to 45.8%) in the 24-hour group had S100B levels below the threshold and theoretically could have been discharged from the ED without a scan.
Discussion
We observed that S100B had good diagnostic ability to rule out significant intracranial pathology in patients presenting to the ED within 6 hours of injury. Theoretically, a quarter of CT-head scans could be avoided and one-fifth of patients could be discharged without waiting for a CT-head scan if S100B was used in addition to the NICE HIGs, with <1% risk of missing a significant injury. Within 24 hours, S100B still had a high NPV but was much less sensitive and the risk of missed injury increased to 2%.
The 6-hour data in this study are consistent with international data,12 demonstrating the diagnostic ability of S100B to exclude intracranial pathology within 6 hours was between 83% and 99% sensitivity with an NPV of 87.5%–100%. It is worth noting that these studies vary somewhat clinically in terms of included population and CT decision threshold. This study has attempted to add to existing literature by focusing the use of S100B to a low-risk cohort of patients where S100B could be targeted to add the most clinical and economic value. All patients in this study had GCS 15, had no diagnosed PTA and were able to consent for themselves at the time of recruitment and would thus be most likely to benefit in terms of shorter stays and faster discharge.
Regarding the false negative results or rather the ‘missed injuries’, one case was identified within the 6-hour time frame. The case was an 86-year-old woman on dabigatran who had suffered a ground-level fall. Her CT scan showed a pinpoint haemorrhage in the left frontal lobe reported to be a contusion. Her case was discussed with the neurosurgical team who advised no intervention. She was observed by the medical team for 24 hours with no further deterioration and discharged after the observation period. Within the 24-hour time frame, five additional cases would have been missed: two men aged 97 and 82 years old on aspirin who sustained small subdural bleeds; a 67-year-old woman with a small subarachnoid bleed; a 34-year-old man with a small contusion and a 47-year-old woman with a tiny contusion. All cases were discussed with neurosurgery and no neurosurgical input was required with the exception of further investigation for the 47-year-old woman to rule out a glioma. Subsequently, this was confirmed to be a small traumatic contusion that required no further intervention. The elderly patients (>65 years) were admitted to medical wards to investigate and manage the cause of their falls. The 34-year-old man was discharged from the ED.
There is no consensus regarding the definition of a clinically significant injury from an ED perspective. Currently, international guidelines, including NICE HIG, recommend admitting all patients with traumatic CT abnormalities.23 One could argue only those requiring neurosurgical intervention are injuries of clinical significance. However, this requires further consideration. Currently, it seems prudent to suggest S100B performed within 6 hours of injury is the safest option.
What rate of missed injury will be viewed as acceptable by clinicians and patients is another conundrum. Not only does individual patient exposure to radiation matter,24 25 but the wider risk to ED attendees who present to crowded departments is important.26 27 ED crowding increases mortality for all conditions,26 27 and waits for CT-head scan can delay intervention for those with injuries.7 Often those with negative CT scans are suffering from concussion,28 29 and waiting in the stimulating ED environment likely exacerbates concussive symptoms. Reduced CT-head rates would potentially benefit departments in terms of reduced crowding, reduced resource load and reduced healthcare costs. From a patient’s perspective, the potential benefits include shorter waits, earlier intervention and earlier discharge. Although crowding was not directly measured, patients on average waited 2.5 hours for CT scans in the ED and only 50% were discharged within the recommended 6-hour LOS target. Theoretically, use of S100B in our clinical setting could reduce CT-head request rates and enable early discharge in this low-risk group.
Limitations
There are several limitations in our current study. First, the consent process is not reflective of how the biomarker would be used during real-time clinical application. It was common for patients to be consented following their CT scan rather than at the decision point for CT-head, which may affect the applicability of the results. In this study, only 50% of the target population had S100B tested within 6 hours of injury as there was not always a trained investigator present to obtain consent. If biomarker testing were part of routine care, this proportion would most certainly increase. Furthermore, ideally, samples need to be processed within 2–4 hours of blood collection, something that most certainly would occur if used in a real-time clinical model. As mentioned in the Methods section, stability has been demonstrated up to 72 hours post-collection for research or prehospital purposes. In this study, 20% of samples were processed within 2 hours, 25% within 4 hours, 63% within 24 hours and 77% within 48 hours. This may affect the accuracy of the biomarker results.
This study only included patients who had GCS 15, had no PTA and were able to consent to the study, therefore these results are only generalisable to this population. Notable groups our inclusion criteria missed include those with reduced GCS because of intoxication, elderly patients with dementia, post-ictal phases of generalised seizures and those with mental health conditions. There is also a low pretest probability of finding an intracranial injury which means that the overall number of positive CT-head scans in the study is low. If the prevalence of positive CT-head increased, this would reduce the NPV of S100B.
An interesting demographic observation noted in the present study is the loss of typical bimodal age distribution. Classically, there is a peak of TBI in the cohort aged 18–35 years and a further peak in the elderly.23 24 In our study, the peak in the younger cohort is not seen, although on review of those excluded, it was notably the younger cohorts who did not consent to a blood test or were unable to consent due to intoxication. The other notable clinical observation is the absence of any positive CT-head scans with an extradural haemorrhage (EDH). Pathologically, initially, this injury may not be associated with brain injury in the early stages but as the haematoma expands, brain injury will occur. Theoretically, if S100B was tested too early in this process, it could miss significant injuries. However, studies investigating the use of S100B in Scandinavia27 noted that all EDHs reported in the literature at the time had an S100B level over the current validated threshold.28
Within the current study, we did not exclude patients presenting with polytrauma. As previously mentioned, adipose, muscle and cardiac tissue can all release S100B in response to trauma. This is likely to have increased the rate of false positives observed in our cohort, and clinically this could limit the reduction in CT-head rates. S100B levels can also be affected by poor renal function and increasing age, and potentially a higher S100B threshold could be more appropriate in the over 65 age group.30 Furthermore, a high proportion of patients in this study were on anticoagulation, and although there is no evidence to suggest this affects S100B levels,31 further consideration is required.
Conclusion and future directions
Within 6 hours of injury, S100B performed well as a diagnostic test to exclude significant intracranial pathology in head-injured patients with a very low risk of missed injury. In theory, if used in conjunction with the NICE HIGs, CT-head request rates could be reduced by one-quarter, and one in five patients could be discharged earlier from the ED. Further work will focus on optimising the performance on S100B in patients with isolated head injuries as well as review real-time economic impact.
Data availability statement
Data are available upon reasonable request. All data supporting the findings in this study are available from the author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Health and Disability Ethics Committee of New Zealand (reference number: 20/CEN/5) and endorsed by CCDHB Research Advisory Group for Māori (RAG-M) (#722). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
This research was supported by a Wellington Medical Research Foundation Grant; Capital and Coast and Hutt Valley District Health Boards & Research Offices; Wellington and Hutt Hospital EDs; the University of Otago (Wellington); a Clinical Research Training Fellowship, Health Research Council of New Zealand, Auckland, New Zealand (22/031 (to AR)); the New Zealand Emergency Medicine Network and the Australasian College for Emergency Medicine Emergency Department Epidemiology Network (ACEM EDEN). The authors would like to thank all the ED clinicians and students who assisted with study promotion and patient recruitment at the study sites, in particular: Catherine Smith, Dr Sinead O’Dwyer, Dr Luke Hayward, Dr Annika Metua and Dr Sanjay Patel. A further special mention to the University of Otago Laboratory Scientists: Bianca Black, Rachelle Smith and Rhiannon Sexton who have contributed to teaching and performing the processing and storage of samples included in this study.
References
Footnotes
Handling editor Jason E Smith
Twitter @alicerogo
Collaborators Endorsed by the Australasian College of Emergency Medicine Emergency Department Epidemiology Network (ACEM EDEN).
Contributors Study design by AR, DM and PDL. Data collection by AR, AS, VP, ED, BP and DM. Blood processing and storage by AR and AS. Data inputting to REDCap was by AR. Data analysis by AR, DM and PDL. Data interpretation, presentation and manuscript writing conducted by all authors. AR is the author responsible for the overall content as the guarantor.
Funding This research was funded by a Wellington Medical Research Foundation Grant and a Clinical Research Training Fellowship, Health Research Council of New Zealand, Auckland, New Zealand (22/031 (to AR)).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.