Article Text

Statistics from Altmetric.com
An 11 year old boy was brought to accident and emergency by ambulance with a history of having been struck by a “ricochet” from a 0.22 inch air rifle fired from approximately 10 metres away by a friend. He had reportedly been clammy at scene, but on arrival at hospital was undistressed, with an oxygen saturation of 100% on oxygen, pulse 100 per minute with no ectopic beats and blood pressure 108/57 mm Hg. A 0.5 cm wound was noted on the right anterior chest wall at the 3rd intercostal space with no palpable underlying pellet.
A chest radiograph (fig 1) demonstrated a pellet within the mediastinum, with a lateral view (fig 2) confirming this to be intracardiac. Computed tomography was performed (fig 3), which showed a small haemothorax and haemopericardium with the pellet lodged between the atria. No pneumothorax was seen, although the track of the pellet through the right lung was noted. The ECG was normal.
He was transferred to the regional paediatric cardiothoracic unit where he underwent emergency surgery using cardiopulmonary bypass and atriotomy to remove the pellet. There was a tense haemopericardium and the pellet was found lodged within but not completely penetrating the intra-atrial septum.
He made a good postoperative recovery and was discharged home after six days. The power of legally available air weapons often appears to be underestimated. Weapons with muzzle velocities of up to 260 m/s are available without licence in the United Kingdom to those aged over 17 years, even although it has previously been estimated that the impact velocity of a 0.22 pellet required to penetrate skin is only in the region of 75 m/s.1 This case serves as a reminder of the potential of such weapons to cause life threatening injuries. Previous reports have illustrated the ability of air gun pellets to embolise from the heart as well as to cause arrhythymias2,3 so consideration needs to be given to emergent removal with careful monitoring for potential complications.
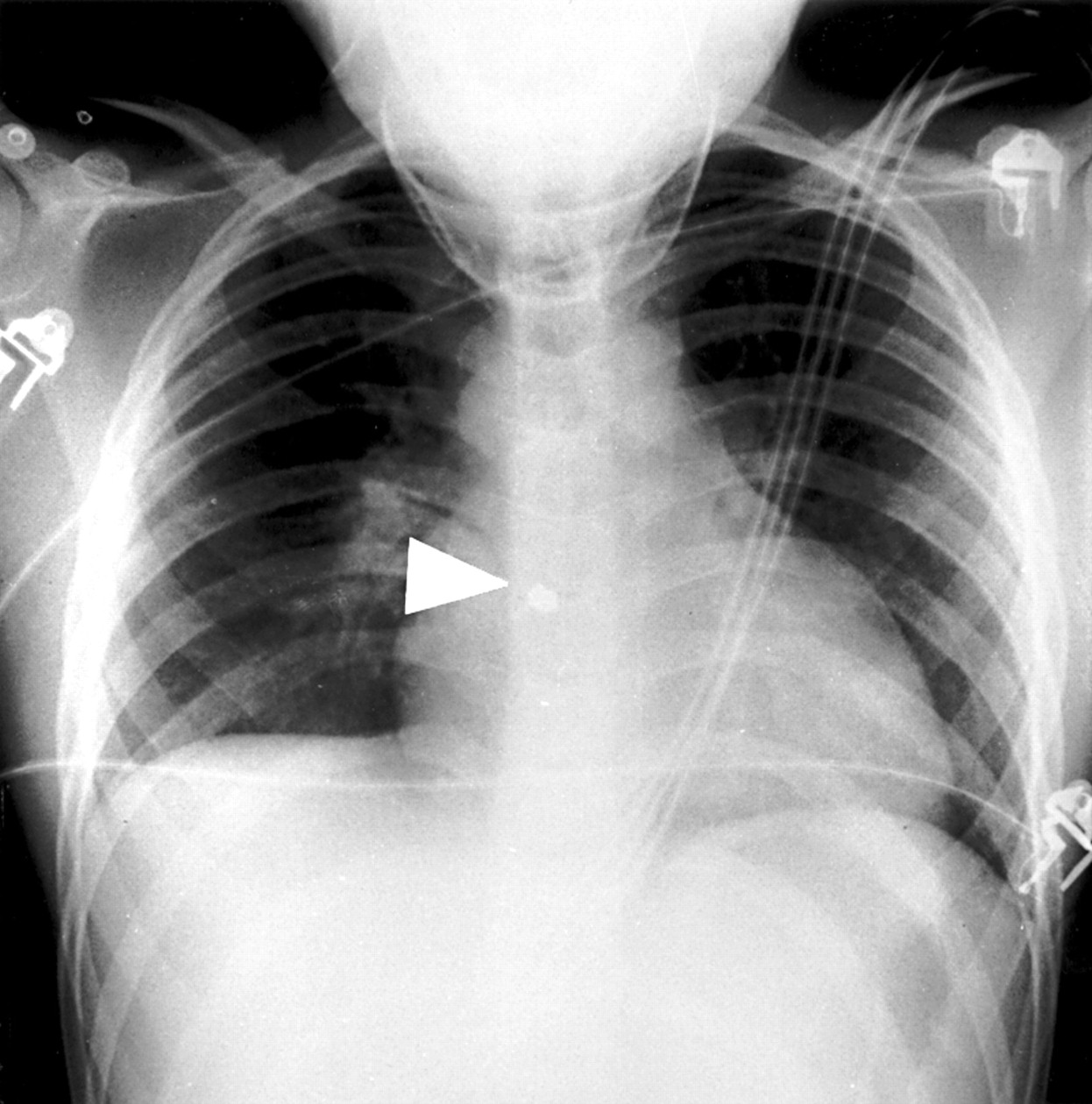
Anteroposterior chest radiograph with pellet (indicated by arrow) seen in mediastinum.

Lateral chest radiograph demonstrating pellet (indicated by arrow) within cardiac shadow.

{kind=link}
{kind=link}
{kind=link}
Thoracic computed tomography showing pellet within intra-atrial septum (narrow arrowhead) and missile track (broad arrowhead) through right lung.
Acknowledgments
Contributors
Tony Hudson and Jonathan Wyatt were both responsible for the initial management of the patient and initiated the report. The literature search was jointly undertaken and Tony Hudson wrote the report. Tony Hudson is the guarantor for this paper. Funding: none. Conflicts of interest: none.
Footnotes
-
Funding: none.
-
Conflicts of interest: none.